








 超级会员免费看
超级会员免费看

 本文探讨了Body-Focused Repetitive Behaviors(BFRBs)如皮肤剥蚀、拔毛等的危害,如感染、疤痕,以及针对智障人士的治疗难题。研究表明,习惯逆转疗法可能无效,但简化版的干预如意识训练和竞争反应训练能减少这些行为。功能分析显示,这些行为通常由自动强化维持。惩罚和意识增强设备(AED)可能作为有效治疗手段,AED通过增强行为意识并提供积极惩罚。在选择治疗时,应考虑行为严重性、消费者价值观和强化策略的结合使用。
本文探讨了Body-Focused Repetitive Behaviors(BFRBs)如皮肤剥蚀、拔毛等的危害,如感染、疤痕,以及针对智障人士的治疗难题。研究表明,习惯逆转疗法可能无效,但简化版的干预如意识训练和竞争反应训练能减少这些行为。功能分析显示,这些行为通常由自动强化维持。惩罚和意识增强设备(AED)可能作为有效治疗手段,AED通过增强行为意识并提供积极惩罚。在选择治疗时,应考虑行为严重性、消费者价值观和强化策略的结合使用。

DOI:10.1007/978-3-319-27297-9_6
Body-focused repetitive behaviors,
including skin picking, skin biting, nail biting, hair pulling, mouth chewing, thumb and finger sucking, and lip biting, arebehaviors that involve repetitive movements centered around the body (Teng et al.2002). These behaviors have the potential to be health and life threatening, producing consequences such as infection, scarring, and other tissue damage (Woods
et al. 2001). Skin picking may cause infections that require treatment by antibiotics and tissue damage that requires skin grafts (Odlaug and Grant 2008). Hair pulling may result in serious health complications including hair follicle damage, carpal tunnel syndrome, and even gastrointestinal and dental problems when the hair is pulled and subsequently consumed (Rapp et al. 2000a, b; Woods et al.
2006). Dental problems can also result from body-focused repetitive behaviors such as nail biting, thumb sucking, mouth chewing, and lip biting (Snorrason and Woods 2014; Teng et al. 2002). Not only can body-focused repetitive behaviors produce physical harm, but they also correlate with social distress, stigmatizing perceptions, and lower levels of self-esteem (Joubert 1993; Long et al. 1998; Snorrason and Woods 2014). Body-focused repetitive behaviors occur in people who are typically-developing and people with intellectual and developmental disabilities (IDD) (Lang et al. 2009). Some studies indicate that there is a higher prevalence among people with intellectual disabilities (Didden et al. 2007; Lang et al. 2009; Long et al. 1998). procedures included awareness training, competing response practice, habit control motivation, and generalization training (Azrin and Nunn 1973). Awareness training for nervous habits involves response description in which the client describes and discusses the unique topography of the habit behavior with the therapist. The next step, response detection, involves practice recognizing when the behavior occurs until the client reliably detects each occurrence. An early warning procedure may also be used which requires the client to practice recognizing the earliest movements of the behavior. The client may also be exposed to situation awareness training in which he or she recalls common situations in which the behavior typically occurs. Competing response practice begins with the identification and selection of a response that is incompatible with (competes with) the habit behavior. The client then practices the competing response and engages in the competing response for a few minutes contingent on the occurrence of the habit behavior. Once the competing response is practiced contingent on the behavior or anticipation of the ehavior in treatment sessions, the client is instructed to use the competing response to control the habit behavior outside of the treatment
sessions. Habit control motivation typically includes a habit inconvenience review and social support. Habit inconvenience review highlights how the client’s habit has inconvenienced the client or impaired his or her functioning and well-being. In social support, family or friends of the client are encouraged to prompt the use of the competing response, praise the client’s use of the competing response, and
praise the client’s improved appearance or lifestyle as a result of using the competing response. Finally, generalization training is incorporated into the habit reversal procedure to ensure that treatment effects will be demonstrated in the client’s natural environment.
Although the multi-component habit reversal procedure was shown to be effective in a number of early studies (Azrin et al. 1980a, b, 1982), researchers subsequently evaluated more simplified forms of the procedure (Miltenberger et al. 1998a, b). Simplified habit reversal, consisting of awareness training and competing response training, has successfully decreased and eliminated several habit behaviors in children and adults (Azrin and Peterson 1989; Miltenberger and Fuqua 1985; Miltenberger et al. 1985; Ollendick 1981; Woods and Miltenberger 1995). However, research suggests that habit reversal or simplified habit reversal (hereafter just called habit reversal) may be an ineffective treatment for people with IDD (Miltenberger et al. 1998a, b) because some of the components of habit reversal may require a higher level of functioning or motivation to be successfully completed. In particular, the competing response component is a self-management procedure that must be implemented contingent on the habit behavior across the client’s day without direct intervention by staff or parents. In addition, the success of the competing response component is predicated on the success of awareness training and the client’s motivation to decrease the habit behavior. Although habit reversal may be ineffective for persons with IDD due to limited skills or motivation, habit reversal may be an effective intervention for people with IDD if it is modified or supplemented with additional procedures (Cavalari et al. 2013; Conlea and Klein-Tasman 2013). Efforts to implement habit reversal procedures with individuals with intellectual disabilities typically require supplemental intervention components such as prompting, differential reinforcement, and response cost
(Cavalari et al. 2013; Long et al. 1999; Miltenberger et al. 1998a, b). In addition,given the limited success of habit reversal, other behavioral interventions have been evaluated for habit behaviors exhibited by individuals with intellectual disabilities. This chapter will highlight research findings on interventions for treating body-focused repetitive behaviors and recommend best practices for clinical treatment with people with intellectual disabilities.
Function of Body-Focused Repetitive Behaviors
Identifying the function of problem behavior is important and often necessary for deciding on best treatment practices. Functional treatments, those that address the antecedents and consequences maintaining the problem behavior, are typically the most successful in achieving desired behavioral outcomes. Furthermore, they are comprised of positive practices rather than aversive procedures (e.g., Kurtz et al.
2003; Neef and Iwata 1994; Pelios et al. 1999). Rapp et al. (2000a, b) suggest that identifying the conditions under which habit behaviors are likely to occur contributes to development or selection of an intervention most likely to be effective, particularly with individuals with IDD whom may not respond to interventions (habit reversal) used with a typically developing population. Studies that have conducted
functional analyses for various habit behaviors have determined that the function is commonly automatic reinforcement (Cowdery et al. 1990; Deaver et al. 2001; Ellingson et al. 2000; Miltenberger et al. 1998a, b; Rapp et al. 1999, 2000a, b; Roscoe et al. 2013). The majority of studies evaluating treatments for body-focused repetitive behaviors that do not conduct a functional analysis rely on the assumption that the behavior is automatically reinforced from the outcome of other functional assessment strategies (e.g., Lang et al. 2009; Radstaake et al. 2011; Rapp et al. 2000a, b). When a behavior is automatically reinforced, it produces a reinforcing consequence directly (not mediated by other individuals) that strengthens and maintains that behavior (Miltenberger 2016). Behaviors maintained by automatic reinforcement tend to be more difficult to treat because you cannot directly modify the contingencies maintaining the behavior and the reinforcement for
engaging in the behavior is constantly available because it results directly from the behavior rather than the actions of others (Piazza et al. 2000). Interventions for automatically reinforced behaviors may involve sensory extinction, achieved by masking the stimulation produced by the behavior, or matching the stimulation produced by the behavior with a more appropriate reinforcer delivered in a noncontingent reinforcement or differential reinforcement procedure (Miltenberger 2016).
Some studies evaluating the effects of particular interventions on body-focused repetitive behaviors suggest that, with the availability of strong reinforcement, addressing the automatic reinforcement function of the behavior may not be necessary. For example, Cowdery et al. (1990) evaluated the effects of a token economy 。
combined with a differential reinforcement of other behavior (DRO) schedule on the self-injurious skin-picking behavior of a 9-year-old boy. Although the subject, Jerry, was not diagnosed with an intellectual disability, he was determined to have low-normal range intelligence and was frequently hospitalized due to the extent of his skin picking and severity of resulting tissue damage. After determining Jerry’s skin-picking to be maintained by automatic reinforcement, a DRO and token reinforcement system was implemented due to the impracticality of implementing interventions involving sensory extinction or matched stimulation for the severe behavior. Jerry earned one penny contingent on each interval in which he did not engage in skin picking while alone in a room with no play activities or tangibles available. Additionally, after the reversal phase, if Jerry earned all five available pennies in a session, he also earned a bonus nickel. Coins were exchanged
for reinforcing activities or items following the conclusion of each session. The DRO intervals were gradually increased from 2 min to 30 min throughout the study. Results indicated that DRO and token reinforcement decreased Jerry’s skin picking to zero or near zero levels across increasing session durations. This study suggests the potential effectiveness of differential reinforcement as an intervention
for body-focused repetitive behaviors using reinforcement that is not functionally related to the behavior of concern.
Despite the finding that interventions for body-focused repetitive behaviors may be effective even if they do not address the antecedents and consequences maintaining the behavior, it is nonetheless prudent to conduct a functional assessment before deciding on intervention. A functional assessment will identify or rule out social reinforcement for the behavior. If the behavior is shown to be maintained by social reinforcement, interventions addressing the social contingencies maintaining the behavior would be warranted. If the behavior is not maintained by social reinforcement, functional analysis procedures to identify the nature of the stimulation reinforcing the behavior would be warranted. Functional interventions might then involve masking the stimulation maintaining the behavior (sensory
extinction) or providing matched stimulation noncontingently or as a reinforcer for alternative behavior (e.g., Rapp et al. 1999, 2000a, b).
Research Findings A variety of interventions have been evaluated for body-focused repetitive behaviors exhibited by individuals with disabilities. These interventions include differential reinforcement (with and without response cost), response interruption,
redirection, and prevention, punishment, and an awareness enhancement device. Differential Reinforcement
Differential reinforcement involves providing a reinforcer for a desirable behavior or for the absence of the problem behavior while withholding reinforcement for the problem behaviors (Miltenberger 2016). Interventions utilizing differential
reinforcement may be effective in decreasing health-threatening habit behaviors for people with intellectual disabilities when used alone or combined with habit reversal. Long et al. (1999) evaluated the effects of habit reversal and habit reversal combined with other interventions on the oral-digital habit behaviors (i.e., nail-biting, finger sucking) of four individuals with intellectual disabilities. The
other interventions included remote prompting, differential reinforcement of nail growth, and differential reinforcement of zero responding (DRO) or differential reinforcement of alternative behaviors (DRA) with response cost. Remote prompting involved the investigator observing the participant through a one-way mirror and verbally prompting the participant through an intercom system to engage in
a competing response when the participant was observed to be engaging in his target behavior. Differential reinforcement of nail growth involved distribution of $5 contingent upon healthy fingernail conditions and uniform nail growth or maintenance of length. In the DRA/DRO and response cost procedure, the participants were instructed not to engage in their target behaviors while the investigator left the room. At the end of a 30-s interval, the investigator delivered one dime or piece of candy if the participants did not engage in the target behavior
(as observed through an observation window) and three dimes or pieces of candy if the participants were executing a competing response when the experimenter reentered the room. Whenever a participant engaged in a target behavior, the investigator entered the room, prompted the competing response, removed a dime or piece of candy, and reset the interval timer. The interval was increased by 60 s following the delivery of each reinforcer. Habit reversal consisted of awareness training, competing response training,
and social support. Modifications were made to enhance the effectiveness of habit reversal for the participants. In one modification, awareness training was supplemented with a game in which the participants indicated when the experimenters engaged in approximations of their target behaviors. In another modification, the experimenters pushed against the participants’ arms while they approximated their
target behaviors to enhance their awareness of the movements. Despite these procedural modifications, results indicated that habit reversal combined with additional contingencies was more effective than habit reversal alone for all participants. Long
et al. (1999) offer a couple explanations for the ineffectiveness of habit reversal. First, a lack of reinforcement in the participants’ natural environments to maintain their use of the competing responses may have accounted for the failure. Second,
the individuals may have been insensitive to social stigma or other negative consequences that may have occurred contingent on their habit behaviors. These potential factors are important to consider when selecting a treatment for body-focused
repetitive behaviors exhibited by individuals with intellectual disabilities. Other studies support the use of differential reinforcement (DRA and DRO) for the reduction of body-focused repetitive behaviors (e.g., Cavalari et al. 2013; Co dery et al. 1990; Lang et al. 2009; Radstaake et al. 2011; Rapp et al. 2000a, b; Roscoe et al. 2013). In treating body-focused repetitive behaviors, DRA may involve
the manipulation of a small toy or other tangible item that is available non-contingently (Cavalari et al. 2013; Radstaake et al. 2011). Cavalari et al. (2013) employed a token economy with an adolescent diagnosed with autism who engaged in selfinjurious skin picking on her hands and arms. The token economy consisted of red and blue tokens that could be redeemed for preferred leisure activities. The participant received a red token contingent upon each 15-min interval in which she did not engage in skin picking and independently manipulated fidget toys that were available non-contingently at her desk in her classroom. She earned a blue token following each 15-min interval in which she engaged in skin picking and manipulated the fidget toys immediately following prompting from staff. The authors referred to the use of fidget toys as a competing response because it was an incompatible behavior to skin picking. In a treatment fading phase, the interval for token reinforcement was increased to 30 min, the fidget toys were removed, and the staff provided praise for
“calm hands” when the participant was not engaging in skin picking and ignored instances of skin picking. Fewer instances of skin picking were observed during this intervention and the results maintained during treatment fading and months following the intervention as reported by staff. Radstaake et al. (2011) also utilized differential reinforcement with an adolescent with Prader-Willi syndrome and mild to moderate intellectual disability who engaged in skin picking. She was exposed to two alternative behaviors to skin picking which the authors refer to as differential reinforcement of incompatible behavior (DRI) and DRA. The DRI behaviors were squeezing a small toy with
both hands and completing a puzzle. The DRA behavior was requesting lotion to apply to her skin. Caregivers prompted the incompatible and/or alternative behavior contingent upon occurrences of skin picking, situations in which skin picking had previously been observed, and when the participant reported feeling compelled to pick her skin. Meetings with the authors were also arranged throughout
the study to rehearse the alternative behaviors and evaluate the condition of her wounds caused by skin picking. Additional praise and small tangible reinforcers were available for attending meetings and more preferred reinforcers were available for noticeable healing of wounds and absence of new wounds. To establish the effectiveness of the procedure, outside observers categorized pictures of the
participant’s skin from the beginning to the end of the study into a correct timeline (i.e., before treatment, after treatment). Results indicated that the differential reinforcement treatment successfully reduced skin picking and increased healing of wounds.
For body-focused repetitive behaviors that involve one’s hands and fingers, such as skin picking, hair pulling, or hand mouthing, manipulating a toy or item with both hands is not only a behavior that is an alternative to the habit, but also a behavior that is incompatible with the habit. In one case, Ladd et al. (2009) reduced self-injurious skin picking in a young girl with autism using only noncontingent access to toys during times in which skin picking was likely to occur. The authors attribute the behavioral reduction to the alternative source of sensory stimulation provided by the toys or to the incompatibility between skin Yicking and manipulating the toys. Similarly, Realon et al. (1995) reduced selfinjurious hand mouthing in an adolescent with a profound intellectual disability
simply by providing access to preferred leisure items.Interventions using differential reinforcement typically require implementation
by others who monitor the target behavior and provide the reinforcer contingent on an alternative behavior or on the absence of the problem behavior. However,Tiger et al. (2009) demonstrated maintenance of treatment effects with an individual diagnosed with Asperger syndrome who engaged in self-monitoring of DRO contingencies for his severe skin picking. After a therapist-monitored DRO
intervention reduced skin picking to 0 % of intervals, the participant maintained the behavioral reduction by successfully monitoring session intervals, identifying occurrences and nonoccurrences of skin picking, and delivering reinforcement according to his token economy. The results of this study indicate the potential for self-monitoring and differential reinforcement to be used by people with intellectual disabilities who engage in body-focused repetitive behaviors. However, the self-managed intervention was used with one individual with Asperger syndrome, so more research is needed to establish the generality of this type of intervention for individuals with varying types and levels of disabilities. The success of differential reinforcement suggests that it may be an effective and acceptable treatment for reducing body-focused repetitive behaviors in individuals with intellectual disabilities. Differential reinforcement presents opportunities to use a positive approach to reduce these potentially health-threatening behaviors. If not employed as a stand-alone procedure, differential reinforcement
should be a component of any other intervention for body-focused repetitive behaviors in individuals with disabilities.
Response Interruption, Redirection, and Prevention Response interruption, redirection, and prevention have been used to decrease several types of behaviors including body-focused repetitive behaviors in people with IDD (Lydon et al. 2013). Response interruption and redirection are commonly used to treat stereotypies maintained by automatic reinforcement, but these procedures may also be useful for treating body-focused repetitive behaviors that are maintained by automatic reinforcement. Response interruption involves stopping a
response someone is engaging in by physically blocking it with a body part (e.g., the hands) and response redirection involves physically prompting an alternative response (Lydon et al. 2013). Response prevention involves preventing a behavior before it occurs through physical restraint or physical barriers (Van Houton and Rolider 1984). In the case of body-focused repetitive behaviors, response prevention typically involves the application of some device, equipment, or garment as a physical barrier to the body part used to engage in the behavior (e.g., Deaver et al. 2001; Maguire et al. 1995). For example, Deaver et al. (2001) used response prevention when they placed thin cotton mittens on a preschool child’s hands to prevent her from engaging in hair pulling during nap times. After first conducting
a functional analysis and ruling out social reinforcement for the behavior, Deaver et al. implemented the response prevention intervention at home and at daycare (see Fig. 6.1). The use of mittens eliminated hair twirling (the precursor to hair pulling) each time it was implemented at nap time in the preschool and bedtime in the home. In another example, Rapp et al. (2000a, b) used a hand splint to prevent hair pulling by an adolescent with intellectual disability in the evening when she was in bed. Although response interruption and DRO implemented by the mother were effective during the day, because the mother was not able to implement the procedure while the client was in bed, the response prevention procedure was used. This example illustrates the use of response prevention as an adjunct to
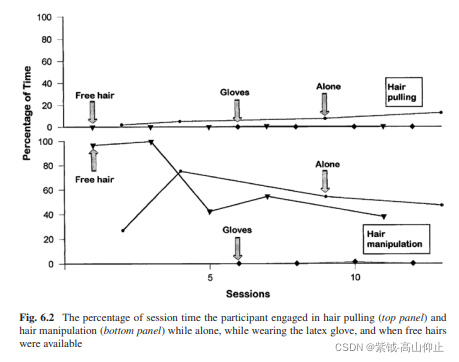
other behavioral intervention procedures that is used only when the caregiver cannot implement the other procedure during specified time periods. More intrusive response prevention interventions have also been used for severe behaviors, such as shaving an individual’s head to prevent hair pulling (Barrett and Shapiro 1980). Response prevention might function by eliminating or attenuating the sensory stimulation that comes from certain body-focused repetitive behaviors and, therefore, may be a functional intervention if the behaviors are in fact maintained by automatic reinforcement. For example, Rapp et al. (1999) showed that a latex glove placed on the hand of a young woman who pulled her hair decreased hair pulling and hair manipulation maintained by sensory stimulation. In this case, the
latex glove masked the sensory stimulation produced by hair manipulation and thus functioned as sensory extinction. As seen in Fig. 6.2, wearing the latex glove eliminated hair pulling (top panel) and hair manipulation (bottom panel). Although response prevention, interruption, and redirection may address the automatic reinforcement function of some body-focused repetitive behaviors, these procedures might also result in behavior reduction through a punishment process. In one study examining chronic trichotillomania in a woman with a profound intellectual disability, the authors used response interruption (referred to by the authors as response correction), which involved a therapist holding the woman’s hands by her side or in her lap for 5 s contingent on occurrences of hair pulling or manipulation (Maguire et al. 1995). This procedure is similar to those used in other studies with body-focused repetitive behaviors such as self-injurious hand-mouthing (Rapp et al. 2000a, b; Turner et al. 1996). Although the response interruption procedure decreased the behavior, Maguire et al. (1995), showed that an intervention using response prevention, placing mitts on the woman’s hands contingent on occurrences of the target behaviors, was more successful than the response interruption procedure. In the literature, response interruption, redirection, or prevention have typically been combined with other procedures such as differential reinforcement (e.g., McEntee et al. 1996; Rapp et al. 2000a, b). Rapp et al. (2000a, b) implemented response interruption (RI) and differential reinforcement (DRO) for a 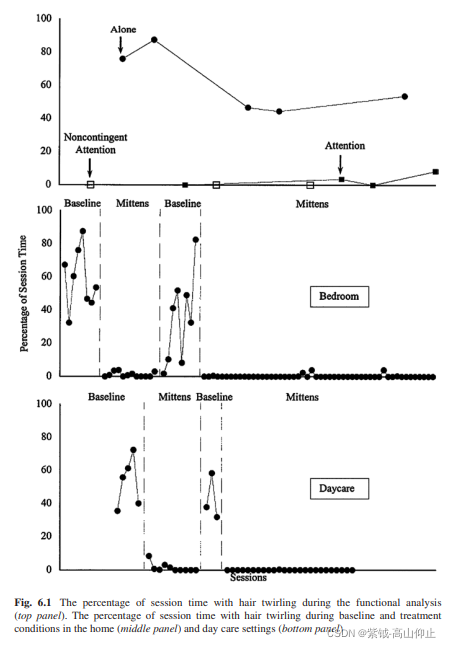
woman with intellectual disabilities after wrist weights and non-contingent application of a glove failed to decrease her hair pulling and hair manipulation over several sessions. Response interruption involved the therapist holding the participant’s arm at her side for 20 s contingent on hair pulling. Differential reinforcement involved the therapist praising the participant’s lack of hair pulling on a
resetting interval schedule that was gradually increased from 30 s to 10 min. The RI and DRO intervention immediately decreased hair pulling and hair manipulation to zero or near zero levels. Furthermore, the treatment effects maintained for several sessions and maintained when the participant’s mother implemented the intervention in the home. The findings from the literature suggest that multi-component interventions including some combination of response interruption, response redirection, response prevention, and differential reinforcement is effective for decreasing body-focused repetitive behaviors. However, the lack of component analyses evaluating individual treatment components leads to uncertainty concerning the utility of any one procedure as a treatment for body-focused repetitive behaviors. We believe an initial evaluation of one of the individual treatment components such as response interruption or redirection may be warranted before moving to multicomponent interventions that require more effort and time to implement. If the individual treatment component is proven effective, additional procedures can be avoided and if proven ineffective, additional procedures can be added.
Punishment Punishment is characterized by a reduction in a behavior when a particular consequence follows the behavior (Miltenberger 2016). The two variations of punishment include positive punishment, in which an aversive stimulus is presented following the behavior, or negative punishment, in which a reinforcing stimulus is removed following the behavior (Miltenberger 2016). Various forms of punishment have been used to reduce body-focused repetitive behaviors in individuals with IDD (e.g., Altman et al. 1978; Barmann and Vitali 1982; Barrett and Shapiro 1980; Corte et al. 1971; Gross et al. 1982). One form of punishment that has been used to decrease body-focused repetitive behaviors is facial screening. Facial screening utilizes the brief application of a bib to cover an individual’s face contingent on the problem behavior. Barmann and Vitali (1982) evaluated the effectiveness of facial screening in the treatment of hair pulling exhibited by three young children with intellectual disabilities. The use of the bib in the intervention did not restrict the children’s breathing and was considered to be an acceptable and ethical intervention by the caregivers. The results indicated that the facial screening procedure decreased hair pulling to zero for all three children. Furthermore, hair pulling remained at zero across several months
for all three children and maintained in an additional school setting for the two children who were in school. Parental reports for two of the children also indicated that tissue damage and bald spots previously resulting from the hair pulling had healed. Because it involves the response-contingent presentation of a stimulus and a subsequent decrease in behavior, facial screening would be considered a form of
positive punishment. Overcorrection is another form of positive punishment that has been used to decrease body-focused repetitive behaviors. In the overcorrection procedure an effortful response is prompted contingent upon the occurrence of a problem
behavior (Miltenberger 2016). In the literature on body-focused repetitive behaviors exhibited by individuals with IDD, successful examples of overcorrection include an oral hygiene procedure involving teeth and gum brushing with antiseptic solution for chronic hand mouthing (Foxx and Azrin 1973) and a hair brushing procedure for hair pulling (Barrett and Shapiro 1980). Because overcorrection
requires an effortful response that is related to the topography of the undesired behavior or the effect of the behavior on the environment, it might be seen as an acceptable form of punishment. Other positive punishment procedures for bodyfocused repetitive behaviors, such as contingent aromatic ammonia and electric shock (Altman et al. 1978; Corte et al. 1971), may not be deemed as acceptable.
Although Corte et al. (1971) showed that contingent electric shock eliminated selfinjurious body-focused repetitive behaviors in individuals with IDD, shock is generally seen as an unacceptable or even unethical procedure and thus unlikely to be used in contemporary practice (Miltenberger et al. 1989). Altman et al. (1978) used contingent aromatic ammonia to reduce hair pulling in a young girl with cerebral palsy, and finger biting in a young boy with a moderate intellectual disability. The procedure involved waving an open ammonia capsule near the participant’s nose contingent on the problem behavior. Altman et al. found the procedure to be effective in reducing the young girl’s hair pulling across several settings when applied for 3 s and in reducing the young boy’s finger biting when applied for 1 s. These results suggest that varying durations of contingent ammonia exposure may be effective in decreasing body-focused repetitive behaviors. However, similar to the use of shock as an intervention, the use of aromatic ammonia is likely to be judged unacceptable in contemporary practice. If even considered at all, the use of such a procedure would be reserved for dangerous and intractable body-focused repetitive behavior. Similar to other interventions used to treat body-focused repetitive behaviors, punishment has been used in combinations with other procedures such as differential reinforcement (Altman et al. 1978; Gross et al. 1982). For example, Gross et al. (1982) evaluated the effects of two combination interventions on the hair pulling in a young boy with cerebral palsy and intellectual disability. These interventions were overcorrection and facial screening, each combined with differential reinforcement of other behavior (DRO). In both procedures, praise was delivered contingent upon each 10-s period that passed with no instances of hair pulling. In the DRO and overcorrection procedure, the therapist raised the boy’s arms above his head and in front of his body for 2 min contingent upon each occurrence of
hair pulling. During the DRO and facial screening procedure, a bib was placed on the boy’s face for 15 s contingent upon each occurrence of hair pulling. Gross et al. found that both interventions decreased the participant’s hair pulling but that the facial screening procedure was more effective. Furthermore, as the hair pulling decreased to near zero, the child engaged in more appropriate play and participated more in academic activities. In addition, the tissue damage from hair pulling healed by the 6-week follow-up period.
Without a component analysis, only inferences can be made about critical treatment components in studies that utilize a combination of procedures. When treating behavioral excesses that are particularly harmful or health threatening such as
body-focused repetitive behaviors that cause serious tissue damage, it is typically in the best interest of the client to treat the behavior as effectively and efficiently as possible, which may supersede the need to evaluate individual treatment components. Therefore, results from these studies demonstrate effective treatments but do not demonstrate a functional relationship between one component and behavioral reduction.
Awareness Enhancement Device
The awareness enhancement device (AED) is an electronic device designed by Rapp et al. (1998) that emits a tone contingent upon proximity of one’s hand to one’s head. Failure of habit reversal to decrease hair pulling and hair manipulation exhibited by a woman with an intellectual disability led to the development of the AED.
The purpose of the AED was to increase awareness of the occurrence of her target behaviors, prompt the use of a competing response (folding her arms across her chest), and provide an aversive auditory stimulus that functioned as positive punishment. The woman was taught to use her competing response for hair pulling when the tone from the AED sounded. The AED emitted the tone contingent upon her
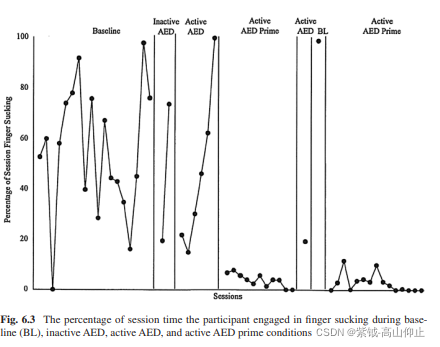
hand moving within 6 in of her head. When the AED was activated, the woman’s hair pulling and manipulation immediately decreased to near zero and subsequently maintained at zero or near zero levels. Other studies have demonstrated similar effects using the AED with thumb sucking (Stricker et al. 2001) and finger sucking (Ellingson et al. 2000). One study used the AED to reduce the finger sucking of a young girl diagnosed with attention deficit disorder and found that the AED alone did not eliminate finger sucking (Stricker et al. 2003). However, the addition of a remote-controlled buzzer to the AED and an increase in the decibel level of the buzzer immediately reduced
finger sucking to zero and maintained zero or near zero levels of finger sucking in the weeks following treatment. As seen in Fig. 6.3, following baseline and a phase in which the child wore the AED without it being activated (Inactive AED), the use of the AED did not decrease the behavior (active AED). Once the additional buzzer was added (Active AED prime), finger sucking decreased to low levels.
As the name implies, the tone emitted by the AED enhances awareness of the target behaviors as they occur. If the participant has learned a competing response, the tone may then prompt the use of the competing response. The tone emitted by the AED may also function as a positive punisher for the precursor movement of the behavior, making the habit behavior less likely to occur. In addition, moving
the hand away from the head may be negatively reinforced by the termination of the tone (Rapp et al. 1998). Regardless of its function, the AED appears to be an effective treatment for reducing health-threatening body-focused repetitive behaviors, and shows promise for individuals with intellectual disabilities. Himle et al. (2008) maintain that being aware of the precursor movements to habit behaviors,
the situations in which habit behaviors are likely to occur, and the functions of habit behaviors are necessary for habit reversal to be successful. This emphasis on the importance of awareness may be one explanation for the ineffectiveness of habit reversal with individuals with intellectual disabilities. In addition, it suggests that an automated intervention such as the AED that does not require awareness of the behavior, or a skill set needed to implement a competing response, or the presence of a care giver to implement contingencies, may be desirable intervention for body focused repetitive behaviors exhibited by individuals with IDD. More
research is warranted to establish the effectiveness and generality of the AED as a stand-alone procedure and as an adjunct to habit reversal for individuals with IDD. Practice Recommendations So far we have described five evidence-based practices that have been used to treat body-focused repetitive behaviors in individuals with intellectual disabilities: habit reversal, differential reinforcement, response interruption, redirection, or prevention, punishment, and the awareness enhancement device. These interventions have been proven to be effective to some extent in reducing or eliminating body-focused repetitive behaviors with this population. This section will review
these interventions and offer recommendations for treatment selection in clinical practice.
Habit reversal is one of the most effective treatments for nervous habits and tics in individuals without disabilities (Miltenberger et al. 1998a, b; Woods and Miltenberger 1995). Habit reversal facilitates increased awareness of the undesired behavior and the use of competing responses to replace the undesired behavior (Azrin and Nunn 1973). Unfortunately, research suggests that habit reversal is not
generally effective for individuals with IDD (e.g., Rapp et al. 1998). The limited effectiveness of habit reversal for people with IDD may be due to a lack of reinforcement in the natural environment for use of competing responses, a lack of motivation to decrease habit behaviors, or difficulty becoming aware of the undesired behaviors (Long et al. 1999). Habit reversal may be successful in reducing
body-focused repetitive behaviors if the client is motivated to change his or her behavior and is affected by social consequences of the behavior. Motivation to change is likely a product of the inconvenience, stigma, or unpleasant social consequences of the behavior. If a client with IDD does not experience these events or is not affected by these events, the client is not likely to be motivated to change the
behavior because decreasing the behavior does not function as a reinforcer. Long et al. (1999) found that habit reversal was most successful for a man diagnosed with mild intellectual disability who expressed displeasure with the appearance of his fingernails due to fingernail biting. This man also reported previous selfinitiated attempts to stop biting his fingernails. Although additional contingencies
were needed to eliminate his fingernail biting, habit reversal reduced the amount of time he engaged in the behavior. It may be beneficial to utilize habit reversal in a clinical setting if the client expresses motivation to stop his or her habit behavior.
When appropriate, habit reversal is a desirable intervention because once the competing response is learned, the client can implement the competing response in his or her natural environment without external contingencies from therapists or caregivers. Habit reversal may promote functional independence, which is in the best interest of individuals receiving treatment. However, more research is needed to
determine when habit reversal may be effective with individuals with intellectual disabilities and which adjunct procedures may enhance its effectiveness. Differential reinforcement has been used in several studies to treat bodyfocused repetitive behaviors in individuals with IDD (e.g., Cavalari et al. 2013;
Cowdery et al. 1990; Lang et al. 2009; Radstaake et al. 2011; Rapp et al. 2000a, b; Roscoe et al. 2013). It has been used alone and in conjunction with other interventions such as habit reversal. Differential reinforcement may take different forms including DRA, DRI, or DRO. Differential reinforcement may also be modified for specific uses related to the behavior, such as differential reinforcement of
nail growth used for clients who engage in finger biting (e.g., Long et al. 1999).
Differential reinforcement uses principles of positive reinforcement to increase the desired behavior and extinction to decrease the undesired behavior. Differential reinforcement is both an effective and acceptable treatment. In addition, there are
opportunities to incorporate the client’s preferences and choices into treatment through the selection of reinforcers for desired behaviors and through the selection of alternative or incompatible behaviors to be reinforced (Radstaake et al. 2011).
Consideration of a client’s preferences and choices is desirable when developing an intervention that will generalize to the client’s natural environment. Although differential reinforcement has several advantages, one disadvantage may be that it can be difficult to implement. Differential reinforcement typically requires implementation by others who are responsible for observing the client, delivering the appropriate reinforcer contingent upon occurrences of desired behavior or non-occurrence of the target behavior, and withholding the reinforcer contingent upon occurrences of the target behavior. The monitoring requirements may involve an unacceptably high level of response effort for those implementing the intervention, which is important to consider especially, when treatment must
be implemented by parents, teachers, or staff. Self-monitored and self-managed differential reinforcement may be a viable alternative to traditional differential reinforcement procedures; however, more research is needed to determine if it is effective with individuals with varying levels of intellectual disabilities. Response interruption, redirection, and prevention are interventions that involve interrupting the behavior early in the sequence, redirecting to a desired alternative behavior, and preventing undesirable behaviors through the application of physical restraints or barriers on the body. These methods have been used alone and combined with differential reinforcement to reduce body-focused repetitive behaviors such as hand mouthing, hair pulling, and hair manipulation. Although not considered functional interventions that address the reinforcing consequence for the behavior, response prevention may be functional if it masks the reinforcing
stimulation arising from the behavior and response redirection may be functional if the client is directed to manipulate stimuli that are matched to the stimulation produced by the repetitive behavior (e.g., Rapp et al. 1999) Only one study directly addressed the automatic reinforcement function of body-focused repetitive behavior (hair pulling) by masking the stimula tion through the use of latex gloves
(Fig. 6.2) and providing stimuli for the client to manipulate that were matched to the stimulation arising from hair pulling (Rapp et al. 1999). Figure 6.2 shows the effects of providing matched stimulation on hair pulling and hair manipulation. When the client had “free hair” she no longer pulled her hair and manipulated the free hair instead of pulling hair and manipulating it. The difficulty associated with the requirement of continuously monitoring a client’s behavior when using differential reinforcement also arises with response
interruption and redirection, in which the implementer must continuously observe the client in order to interrupt and redirect the behaviors when they occur. This difficulty could present a disadvantage to using response interruption and redirection with body-focused repetitive behaviors. However, response prevention in the form of applying gloves or splints to the hands of clients engaging in hand
mouthing or hair pulling decreases the behaviors through simple barriers or in some cases by addressing the sensory stimulation function. Furthermore, because it does not require social mediation, it is a procedure that can be used when staff
cannot be continuously present with the client or when the client is alone (Deaver et al. 2001; Rapp et al. 2000a, b). The use of response prevention devices such as gloves or hand splints should be discussed with the caregivers (as should any intervention) to establish the acceptability of the procedure. Furthermore, a treatmentfading plan should be developed with the goal of eliminating the use of the barrier
devices. Another intervention that does not require implementers to be continuously present in the environment with the client is the Awareness Enhancement Device (AED). As described previously, the AED is an electronic device that emits a tone
when the wearer moves a hand towards his or her head (it could be programmed to include other body parts or locations as well). Results from the few studies that have evaluated the effectiveness of the AED indicate that it reduces body-focused
repetitive behaviors including hair pulling and thumb sucking by individuals with intellectual disabilities (Rapp et al. 1998; Stricker et al. 2001). The AED promotes acquisition of a replacement behavior, which is negatively reinforced by termination of the buzzer, while decreasing the undesired behavior through positive punishment without a caregiver or staff member being present to monitor the behavior
and implement an intervention (Rapp et al. 2000a, b). The AED is a promising intervention for reducing body-focused repetitive behaviors in individuals with intellectual disabilities. More research is needed that evaluates the effects of the AED across multiple types of health-threatening behaviors and individuals with varying disabilities. The AED enhances awareness of the occurrence of the behavior that produces the tone in addition to arranging automatic negative reinforcement and positive punishment contingencies. Any time punishment is used in an intervention, care must be taken to ensure the individual has access to alternative sources of reinforcement and that the treatment is acceptable to those involved. Forms of punishment used to treat body-focused repetitive behaviors include
facial screening, overcorrection, electric shock, and aromatic ammonia (e.g., Altman et al. 1978; Barmann and Vitali 1982; Barrett and Shapiro 1980; Corte et al. 1971; Gross et al. 1982). Although interventions using intense forms of punishment such as electric shock have been proven to be effective in decreasing selfinjurious behavior (Corte et al. 1971; Favell et al. 1982; Linscheid et al. 1990) we
do not recommend these approaches for body-focused repetitive behaviors due to their limited acceptability and the focus on functional and nonaversive approaches in contemporary practice. When possible, positive interventions should be used
before interventions involving punishment (Bailey and Burch 2011). In recent years the research has moved away from punishment procedures in favor of positive interventions, but more research is needed to identify whether positive interventions are equally effective and if clinical practice follows trends in the research (Matson and LoVullo 2008). (Matson and LoVullo 2008).
When identifying a treatment for body-focused repetitive behaviors, several factors must be taken into consideration including the severity of the behavior and values of the consumer. If the behavior is severe or life threatening, it may be necessary to use punishment if it will yield the most efficient reduction in the behavior. Punishment may also be a necessary component of an intervention if positive practices fail to reduce a health-threatening behavior to an acceptable level. However, punishment should always be combined with reinforcement procedures such as differential reinforcement or noncontingent reinforcement (Lerman and Vorndran 2002). As in any treatment selection process, the advantages and disadvantages of punishment should be considered. For example, although contingent aromatic ammonia was effective in decreasing hair pulling and hand biting in a study by Altman et al. (1978), several issues arose during implementation including difficulty of administration due to social stigma, environmental challenges, changing topographies of behavior, and difficulty monitoring and identifying occurrences of the behavior. Ultimately, we do not recommend punishment involving the application of aversive stimulation due to current philosophies in the field, limited acceptability, and the availability of effective, less intrusive procedures.
Practitioners should evaluate the needs of their specific client and determine what is best based on the behavior of concern, the values of the consumer, ethical guidelines, and empirical support from the literature.
References
Altman, K., Haavik, S., & Cook, W. (1978). Punishment of self-injurious behavior in natural settings using contingent aromatic ammonia. Behaviour Research and Therapy, 16, 85–96.
Azrin, N. H., & Nunn, R. G. (1973). A method of eliminating nervous habits and tics. Behaviour Research and Therapy, 11, 619–628.
Azrin, N. H., Nunn, R. G., & Frantz, S. E. (1980a). Habit reversal versus negative practice treatment of nailbiting. Behaviour Research and Therapy, 18, 281–285. Azrin, N. H., Nunn, R. G., & Frantz-Renshaw, S. E. (1980b). Habit reversal treatment of thumbsucking. Behaviour Research and Therapy, 18, 195–399. Azrin, N. H., Nunn, R. G., & Frantz-Renshaw, S. E. (1982). Habit reversal versus negative practice treatment of destructive oral habits (biting, chewing or licking of the lips, cheeks, tongue or palate). Journal of Behavior Therapy and Experimental Psychiatry, 13, 49–54. Azrin, N. H., & Peterson, A. L. (1989). Reduction of an eye tic by controlled blinking. Behavior
Therapy, 20, 467–473. Bailey, J., & Burch, M. (2011). Ethics for behavior analysts: Second (expanded ed.). New York:
Routledge. Barmann, B. C., & Vitali, D. L. (1982). Facial screening to eliminate trichotillomania in developmentally disabled persons. Behavior Therapy, 13, 735–742. Barrett, R. P., & Shapiro, E. S. (1980). Treatment of stereotyped hairpulling with overcorrection: A case study with long term follow-up. Journal of Behavior Therapy and Experimental Psychiatry, 11, 317–320. Cavalari, R. S., DuBard, M., & Luiselli, J. K. (2013). Simplified habit reversal and treatment fading for chronic skin picking in an adolescent with autism. Clinical Case Studies, 13, 190–198. Conelea, C. A., & Klein-Tasman, B. P. (2013). Habit reversal therapy for body-focused repetitive behaviors in Williams syndrome: A case study. Journal of Developmental and Physical Disabilities, 25, 597–611.
Corte, H. E., Wolf, M. M., & Locke, B. J. (1971). A comparison of procedures for eliminating self-injurious behavior of retarded adolescents. Journal of Applied Behavior Analysis, 4, 201–213.
Cowdery, G. E., Iwata, B. A., & Pace, G. M. (1990). Effects and side effects of DRO as treatment for self-injurious behavior. Journal of Applied Behavior Analysis, 23, 497–506. Deaver, C. M., Miltenberger, R. G., & Stricker, J. M. (2001). Functional analysis and treatment
of hair twirling in a young child. Journal of Applied Behavior Analysis, 34, 535–538. Didden, R., Korzilius, H., & Curfs, M. G. (2007). Skin-picking in individuals with Prader-Willi
syndrome: prevalence, functional assessment, and its comorbidity with compulsive and selfinjurious behaviours. Journal of Applied Research in Intellectual Disabilities, 20, 409–419.
Ellingson, S. A., Miltenberger, R. G., Stricker, J. M., Garlinghouse, M. A., Roberts, J., Galensky,
T. L., & Rapp, J. T. (2000). Analysis and treatment of finger sucking. Journal of Applied
Behavior Analysis, 33, 41–52.
Favell, J. E., Azrin, N. H., Baumeister, A. A., Carr, E. G., Dorsey, M. F., Forehand, R., & Solnick,
J. V. (1982). The treatment of self-injurious behavior. Behavior Therapy, 13, 529–554.
Foxx, R. M., & Azrin, N. H. (1973). The elimination of autistic self-stimulatory behavior by
overcorrection. Journal of Applied Behavior Analysis, 6, l–14.
Gross, A. M., Farrar, M. J., & Liner, D. (1982). Reduction of trichotillomania in a retarded cerebral palsied child using overcorrection, facial screening, and differential reinforcement of
other behavior. Education and Treatment of Children, 5, 133–140.
Himle, J. A., Perlman, D. M., & Lokers, L. M. (2008). Prototype awareness enhancing and monitoring device for trichotillomania. Behaviour Research and Therapy, 46, 1187–1191.
Joubert, C. E. (1993). Relationship of self-esteem, manifest anxiety, and obsessive- compulsiveness to personal habits. Psychological Reports, 73, 579–583.
Kurtz, P. F., Chin, M. D., Huete, J. M., Tarbox, R. S. F., O’Connor, J. T., Paclawskyi, T. R., &
Rush, K. S. (2003). Functional analysis and treatment of self-injurious behavior in young
children: A summary of 30 cases. Journal of Applied Behavior Analysis, 36, 205–219.
Ladd, M. V., Luiselli, J. K., & Baker, L. (2009). Continuous access to competing stimulation as
intervention for self-injurious skin picking in a child with autism. Child & Family Behavior
Therapy, 31, 54–60.
Lang, R., Didden, R., Sigafoos, J., Rispoli, M., Regester, A., & Lancioni, G. E. (2009). Treatment
of chronic skin-picking in an adolescent with Asperger syndrome and borderline intellectual
disability. Clinical Case Studies, 8, 317–325.
Lerman, D. C., & Vorndran, C. M. (2002). On the status of knowledge for using punishment:
Implications for treating behavior disorders. Journal of Applied Behavior Analysis, 35,
431–464.
Linscheid, T. R., Iwata, B. A., Ricketts, R. W., Williams, D. E., & Griffin, J. C. (1990). Clinical
evaluation of the self-injurious behavior inhibiting system (SIBIS). Journal of Applied
Behavior Analysis, 23, 53–78.
Long, E. S., Miltenberger, R. G., Ellingson, S. A., & Ott, S. M. (1999). Augmenting simplified
habit reversal in the treatment of oral-digital habits exhibited by individuals with mental
retardation. Journal of Applied Behavior Analysis, 32, 353–365.
Long, E. S., Miltenberger, R. G., & Rapp, J. T. (1998). A survey of habit behaviors exhibited by
individuals with mental retardation. Behavioral Interventions, 13, 79–89.
Lydon, S., Healy, O., O’Reilly, M., & McCoy, A. (2013). A systematic review and evaluation of
response redirection as a treatment for challenging behavior in individuals with developmental disabilities. Research in Developmental Disabilities, 34, 3148–3158.
Maguire, K., Piersel, W., & Hauser, B. (1995). A long-term treatment of trichotillomania: A case
study of a woman with profound mental retardation living in an applied setting. Journal of
Developmental and Physical Disabilities, 7, 185–202.
Matson, J. L., & LoVullo, S. V. (2008). A review of behavioral treatments for self-injurious
behaviors of persons with autism spectrum disorders. Behavior Modification, 32, 61–76.
McEntee, J. E., Parker, E. H., Brown, M. B., & Poulson, R. L. (1996). The effects of response
interruption, DRO, and positive reinforcement on the reduction of hand-mouthing behavior.
Behavioral Interventions, 11, 163–170.
Miltenberger, R. G. (2016). Behavior modification: Principles and procedures (6th ed.). Pacific
Grove, CA: Wadsworth.
Miltenberger, R. G., & Fuqua, R. W. (1985). A comparison of contingent versus noncontingent
competing response practice in the treatment of nervous habits. Journal of Behavior Therapy
and Experimental Psychiatry, 16, 195–200.
Miltenberger, R., Fuqua, W., & McKinley, T. (1985). Habit reversal with muscle tics: Replication
and component analysis. Behavior Therapy, 16, 39–50.
Miltenberger, R., Fuqua, R., & Woods, D. (1998a). Applying behavior analysis with clinical
problems: Review and analysis of habit reversal. Journal of Applied Behavior Analysis, 31,
447–461.
Miltenberger, R. G., Long, E. S., Rapp, J. T., Lumley, V. A., & Elliot, A. J. (1998b). Evaluating
the function of hair pulling: A preliminary investigation. Behavior Therapy, 29, 211–219.
Miltenberger, R. G., Lennox, D. B., & Erfanian, N. (1989). Acceptability of alternative treatments for persons with mental retardation: Ratings from institutional and community based
staff. American Journal of Mental Retardation, 93, 388–395.
Neef, N. A., & Iwata, B. A. (1994). Current research on functional analysis methodologies: An
introduction. Journal of Applied Behavior Analysis, 27, 211–214.
Ollendick, T. H. (1981). Self-monitoring and self-administered overcorrection: The modification
of nervous tics in children. Behavior Modification, 5, 75–84.
Odlaug, B. l., & Grant, J. E. (2008). Clinical characteristics and medical complications of pathologic skin picking. General Hospital Psychiatry, 30, 61–66.
以身体为中心的重复行为,
包括抓皮肤、咬皮肤、咬指甲、拔头发、咀嚼嘴巴、吮吸拇指和手指以及咬嘴唇,这些行为涉及以身体为中心的重复运动(Teng et al.2002)。这些行为有可能危及健康和生命,产生感染、疤痕和其他组织损伤等后果(Woods
等。 2001)。皮肤采摘可能导致需要抗生素治疗的感染和需要皮肤移植的组织损伤(Odlaug 和 Grant 2008)。拔毛可能会导致严重的健康并发症,包括毛囊损伤、腕管综合征,甚至在拔毛并随后食用时会出现胃肠道和牙齿问题(Rapp 等人,2000a,b;Woods 等人。
2006)。牙齿问题也可能是由以身体为中心的重复行为引起的,例如咬指甲、吮吸拇指、咀嚼嘴巴和咬嘴唇(Snorrason 和 Woods 2014;Teng 等人 2002)。以身体为中心的重复行为不仅会产生身体伤害,而且还与社会痛苦、污名化观念和较低的自尊水平相关(Joubert 1993; Long et al. 1998; Snorrason and Woods 2014)。以身体为中心的重复行为发生在发育正常的人以及智力和发育障碍 (IDD) 的人身上(Lang 等人,2009 年)。一些研究表明,智障人士的患病率更高(Didden 等人,2007;Lang 等人,2009;Long 等人,1998)。程序包括意识训练、竞争反应练习、习惯控制动机和泛化训练(Azrin 和 Nunn 1973)。对紧张习惯的意识训练涉及反应描述,其中客户描述并与治疗师讨论习惯行为的独特地形。下一步,响应检测,涉及练习识别行为何时发生,直到客户端可靠地检测到每个事件。也可以使用早期预警程序,该程序要求客户练习识别行为的最早动作。客户还可能会接受情境意识培训,在培训中他或她回忆起行为通常发生的常见情况。竞争反应练习始于识别和选择与习惯行为不相容(与之竞争)的反应。然后,客户练习竞争反应,并根据习惯行为的发生情况进行几分钟的竞争反应。一旦根据治疗过程中的行为或对行为的预期来实施竞争反应,就指示来访者使用竞争反应来控制治疗之外的习惯行为
会议。习惯控制动机通常包括习惯不便回顾和社会支持。习惯不便审查强调客户的习惯如何给客户带来不便或损害他或她的功能和幸福感。在社会支持方面,鼓励来访者的家人或朋友提示使用竞争性反应,表扬客户对竞争性反应的使用,以及
表扬客户因使用竞争反应而改善的外表或生活方式。最后,将泛化培训纳入习惯逆转程序,以确保在客户的自然环境中展示治疗效果。
尽管多组分习惯逆转程序在许多早期研究中被证明是有效的(Azrin et al. 1980a, b, 1982),但研究人员随后评估了更简化的程序形式(Miltenberger et al. 1998a, b)。简化的习惯逆转,包括意识训练和竞争反应训练,已经成功地减少和消除了儿童和成人的几种习惯行为(Azrin 和 Peterson 1989;Miltenberger 和 Fuqua 1985;Miltenberger 等 1985;Ollendick 1981;Woods 和 Miltenberger 1995) .然而,研究表明,习惯逆转或简化的习惯逆转(以下简称为习惯逆转)可能对 IDD 患者无效(Miltenberger 等,1998a,b),因为习惯逆转的某些组成部分可能需要更高水平的成功完成的功能或动机。特别是,竞争反应组件是一个自我管理程序,必须根据客户一天中的习惯行为来实施,而无需工作人员或父母的直接干预。此外,竞争反应组件的成功取决于意识培训的成功和客户减少习惯行为的动机。尽管由于技能或动机有限,习惯逆转可能对 IDD 患者无效,但如果对 IDD 患者进行修改或补充,习惯逆转可能是一种有效的干预措施。最终程序(Cavalari 等人 2013;Conlea 和 Klein-Tasman 2013)。对智障人士实施习惯逆转程序的努力通常需要补充干预组件,例如提示、差异强化和响应成本
(Cavalari 等人,2013;Long 等人,1999;Miltenberger 等人,1998a,b)。此外,鉴于习惯逆转的成功率有限,其他行为干预措施已针对智障人士表现出的习惯行为进行了评估。本章将重点介绍治疗以身体为中心的重复行为的干预措施的研究结果,并推荐临床治疗智障人士的最佳实践。
以身体为中心的重复行为的功能
识别问题行为的功能对于决定最佳治疗实践非常重要并且通常是必要的。功能性治疗,即那些解决维持问题行为的前因和后果的治疗,通常最成功地实现了预期的行为结果。此外,它们由积极的实践而不是厌恶的程序组成(例如,Kurtz 等人。
2003;尼夫和岩田 1994;佩利奥斯等人。 1999)。拉普等人。 (2000a, b) 表明,识别可能发生习惯行为的条件有助于开发或选择最有可能有效的干预措施,特别是对于可能对干预措施(习惯逆转)没有反应的 IDD 个体典型的发展中人口。已进行的研究
对各种习惯行为的功能分析已确定该功能通常是自动强化(Cowdery 等人 1990;Deaver 等人 2001;Ellingson 等人 2000;Miltenberger 等人 1998a,b;Rapp 等人 1999,2000a, b;Roscoe 等人,2013 年)。大多数评估针对以身体为中心的重复行为的治疗但不进行功能分析的研究依赖于假设行为是从其他功能评估策略的结果中自动得到加强的(例如,Lang 等人,2009 年;Radstaake 等人。 2011;Rapp 等人 2000a, b)。当一种行为被自动强化时,它会直接产生强化后果(不由其他人介导),从而强化和维持该行为(Miltenberger 2016)。由自动强化维持的行为往往更难处理,因为你不能直接修改维持行为的偶然因素和强化
参与行为是持续可用的,因为它直接来自行为而不是他人的行为(Piazza 等,2000)。对自动强化行为的干预可能涉及感觉消退,通过掩盖行为产生的刺激或将行为产生的刺激与在非偶然强化或差异强化程序中传递的更合适的强化物相匹配来实现(Miltenberger 2016)。
一些评估特定干预措施对以身体为中心的重复行为的影响的研究表明,随着强强化的可用性,解决行为的自动强化功能可能没有必要。例如,考德里等人。 (1990) 评估了代币经济的影响。
结合其他行为的差异强化(DRO)时间表对一个 9 岁男孩的自伤皮肤采摘行为。尽管受试者 Jerry 没有被诊断出有智力障碍,但他被确定为低正常范围的智力,并且由于他的皮肤采摘程度和由此产生的组织损伤的严重程度而经常住院。在确定 Jerry 的皮肤采摘将通过自动强化来维持后,由于实施涉及感官消退或对严重行为的匹配刺激的干预措施不切实际,因此实施了 DRO 和令牌强化系统。杰瑞在没有任何游戏活动或有形物品的房间里独自一人不进行皮肤采摘的每个间隔中赚取一分钱。此外,在逆转阶段之后,如果 Jerry 在一个会话中赢得了所有可用的五美分,他还获得了奖金镍。硬币被交换
在每次会议结束后加强活动或项目。在整个研究过程中,DRO 间隔从 2 分钟逐渐增加到 30 分钟。结果表明,随着会话持续时间的增加,DRO 和令牌强化将 Jerry 的皮肤采摘降低到零或接近零的水平。这项研究表明差异强化作为一种干预措施的潜在有效性
对于以身体为中心的重复行为,使用在功能上与关注行为无关的强化。
尽管发现针对以身体为中心的重复行为的干预措施可能是有效的n 如果他们没有解决维持行为的前因和后果,那么在决定干预之前进行功能评估仍然是谨慎的。功能评估将识别或排除行为的社会强化。如果行为被证明是通过社会强化来维持的,则有必要采取干预措施来解决维持该行为的社会突发事件。如果行为不是通过社会强化来维持,则需要使用功能分析程序来识别强化行为的刺激的性质。然后,功能干预可能涉及掩盖维持行为的刺激(感觉
消退)或非偶然地提供匹配的刺激或作为替代行为的强化物(例如,Rapp et al. 1999, 2000a, b)。
研究结果 已经针对残疾人表现出的以身体为中心的重复行为评估了各种干预措施。这些干预措施包括差异强化(有或没有反应成本)、反应中断、
重定向、预防、惩罚和意识增强装置。差异强化
差异强化涉及为理想行为或不存在问题行为提供强化物,同时为问题行为保留强化(Miltenberger 2016)。利用差异的干预措施
当单独使用或与习惯逆转结合使用时,强化可能有效减少智障人士的威胁健康的习惯行为。龙等人。 (1999) 评估了习惯逆转和习惯逆转结合其他干预措施对四名智障人士的口腔数字习惯行为(即咬指甲、吸手指)的影响。这
其他干预措施包括远程提示、指甲生长的差异强化、零响应差异强化 (DRO) 或替代行为差异强化 (DRA) 与响应成本。远程提示涉及调查员通过单向镜子观察参与者,并通过对讲系统口头提示参与者参与
当观察到参与者正在从事他的目标行为时的竞争反应。指甲生长的差异强化涉及根据健康的指甲状况和均匀的指甲生长或长度维持而分配 5 美元。在 DRA/DRO 和响应成本程序中,参与者被指示在调查员离开房间时不要从事他们的目标行为。在 30 秒的间隔结束时,如果参与者没有参与目标行为,则调查员会送出一角硬币或一块糖果
(通过观察窗观察)和三角硬币或糖果,如果当实验者重新进入房间时参与者正在执行竞争反应。每当参与者进行目标行为时,调查员进入房间,提示竞争反应,取出一角硬币或一块糖果,并重置间隔计时器。每次强化物投放后,间隔时间增加 60 秒。习惯逆转包括意识训练、竞争反应训练、
和社会支持。进行了修改以提高参与者改变习惯的有效性。在一个修改中,意识训练辅以一个游戏,参与者在游戏中指出实验者何时参与了他们的目标行为的近似。在另一个修改中,实验者推着参与者的手臂,同时他们接近他们的
目标行为,以增强他们对动作的认识。尽管进行了这些程序上的修改,但结果表明,对于所有参与者,习惯逆转结合额外的意外事件比单独的习惯逆转更有效。长
等。 (1999)对习惯逆转的无效性提供了一些解释。首先,参与者的自然环境缺乏强化来维持他们对竞争反应的使用可能是失败的原因。第二,
个人可能对社会污名或其他可能因他们的习惯行为而发生的负面后果不敏感。在选择以身体为中心的治疗方法时,这些潜在因素很重要
智障人士表现出的重复行为。其他研究支持使用差异强化(DRA 和 DRO)来减少以身体为中心的重复行为(例如,Cavalari 等人 2013;Co dery 等人 1990;Lang 等人 2009;Radstaake 等人 2011; Rapp et al. 2000a, b; Roscoe et al. 2013)。在治疗以身体为中心的重复行为时,DRA 可能涉及
对非偶然可用的小玩具或其他有形物品的操纵(Cavalari 等人。 2013;拉德斯塔克等人。 2011)。卡瓦拉里等人。 (2013 年)与一名被诊断患有自闭症的青少年采用象征性经济,她在手和手臂上进行自伤性皮肤采摘。代币经济由红色和蓝色代币组成,可以兑换成首选的休闲活动。参与者每隔 15 分钟收到一个红色标记,在此期间她没有进行皮肤采摘,并且独立地操纵了她教室办公桌上非偶然可用的坐立不安玩具。她每 15 分钟进行一次皮肤采摘,并在工作人员提示后立即操作这些坐立不安的玩具,她就获得了一个蓝色令牌。作者将使用坐立不安的玩具称为一种竞争性反应,因为它与皮肤采摘行为不相容。在一个治疗消退阶段,令牌强化的间隔增加到30分钟,烦躁的玩具被移除,工作人员给予表扬
当参与者没有进行皮肤采摘并忽略皮肤采摘的情况时,“平静的手”。根据工作人员的报告,在此干预期间观察到的皮肤采摘次数较少,并且在治疗消退期间和干预后的几个月内保持结果。拉德斯塔克等人。 (2011 年)还对一名患有 Prader-Willi 综合征和轻度至中度智力障碍的青少年进行了不同的强化,他们从事皮肤采摘。她接触了两种皮肤采摘的替代行为,作者将其称为不相容行为 (DRI) 和 DRA 的差异强化。 DRI 行为是挤压一个小玩具
双手完成拼图。 DRA 的行为是要求将乳液涂抹在她的皮肤上。护理人员会根据皮肤采摘的发生、之前观察到皮肤采摘的情况以及参与者报告感觉被迫采摘她的皮肤时提示不相容和/或替代行为。还安排了与作者的会面
这项研究旨在排练替代行为并评估她因皮肤采摘造成的伤口状况。额外的表扬和小的有形强化物可用于参加会议,更优选的强化物可用于明显的伤口愈合和没有新伤口的情况。为了确定该程序的有效性,外部观察者对图片进行了分类
参与者的皮肤从研究开始到结束进入正确的时间线(即治疗前、治疗后)。结果表明,差异强化治疗成功地减少了皮肤采摘并增加了伤口的愈合。
对于涉及手和手指的以身体为中心的重复性行为,例如抠皮、拉头发或用手吐口水,用双手操纵玩具或物品不仅是一种替代习惯的行为,而且是一种行为这与习惯不相容。在一种情况下,Ladd 等人。 (2009 年)减少了一名自闭症年轻女孩在可能发生皮肤采摘时仅使用非偶然性接触玩具的自伤皮肤采摘。作者将行为减少归因于玩具提供的感官刺激的替代来源,或皮肤抓挠和操纵玩具之间的不相容性。同样,Realon 等人。 (1995) 减少了严重智力障碍青少年的自残手口吐
只需提供对首选休闲项目的访问权限。使用差异强化的干预通常需要实施
由其他人监控目标行为并根据替代行为或不存在问题行为提供强化物。然而,Tiger 等人。 (2009 年)对一名被诊断患有阿斯伯格综合症的人展示了维持治疗效果,该人对严重皮肤采摘的 DRO 突发事件进行自我监测。在治疗师监测的 DRO 之后
干预将皮肤采摘减少到 0% 的间隔,参与者通过成功监控会话间隔、识别皮肤采摘的发生和未发生以及根据他的代币经济提供强化来维持行为减少。这项研究的结果表明,从事以身体为中心的重复行为的智障人士可以使用自我监控和差异强化的潜力。然而,自我管理干预是针对一名阿斯伯格综合症患者使用的,因此需要更多的研究来确定这种干预对不同类型和残疾程度的个体的普遍性。差异强化的成功表明,它可能是一种有效且可接受的治疗方法,可减少智障人士以身体为中心的重复行为。差异化强化为你提供了机会寻找一种积极的方法来减少这些潜在的威胁健康的行为。如果不作为独立程序使用,差异强化
应该是针对残障人士以身体为中心的重复性行为的任何其他干预措施的组成部分。
响应中断、重定向和预防响应中断、重定向和预防已被用于减少多种类型的行为,包括 IDD 患者的以身体为中心的重复行为(Lydon 等人,2013 年)。反应中断和重定向通常用于治疗由自动强化维持的刻板印象,但这些程序也可用于治疗由自动强化维持的以身体为中心的重复行为。响应中断涉及停止一个
通过用身体部位(例如手)物理阻挡某人正在参与的响应,响应重定向涉及物理提示替代响应(Lydon et al. 2013)。反应预防包括通过物理约束或物理障碍在行为发生之前阻止行为(Van Houton 和 Rolider 1984)。在以身体为中心的重复行为的情况下,反应预防通常涉及应用一些装置、设备或服装作为身体部位的物理屏障(例如,Deaver et al. 2001; Maguire et al. . 1995)。例如,迪弗等人。 (2001 年)他们将薄棉手套放在学龄前儿童的手上,以防止她在午睡时间拉扯头发,从而使用了反应预防。第一次进行后
功能分析并排除行为的社会强化,Deaver 等人。在家庭和日托中心实施了应对预防干预(见图 6.1)。每次在学前班的午睡时间和家中的就寝时间使用连指手套时,都会消除头发旋转(拉头发的前兆)。在另一个例子中,Rapp 等人。 (2000a, b) 使用夹板防止智障青少年在晚上睡觉时拉扯头发。虽然母亲实施的反应中断和 DRO 在白天是有效的,但由于母亲无法在客户躺在床上时实施该程序,因此使用了反应预防程序。此示例说明使用响应预防作为辅助
仅当护理人员在指定时间段内无法实施其他程序时才使用的其他行为干预程序。更具侵入性的反应预防干预措施也被用于严重行为,例如剃光个人的头部以防止头发拉扯(Barrett 和 Shapiro 1980)。反应预防可能通过消除或减弱来自某些以身体为中心的重复行为的感觉刺激来发挥作用,因此,如果这些行为实际上是通过自动强化来维持的,则可能是一种功能性干预。例如,拉普等人。 (1999) 表明,将乳胶手套放在拉头发的年轻女性手上,可减少由感官刺激维持的拉头发和头发操作。在这种情况下,
乳胶手套掩盖了头发操作产生的感官刺激,因此起到了感官消退的作用。如图 6.2 所示,戴上乳胶手套消除了拉头发(上图)和头发操作(下图)。尽管反应预防、中断和重定向可能会解决一些以身体为中心的重复行为的自动强化功能,但这些程序也可能通过惩罚过程导致行为减少。在一项检查患有严重智力障碍的女性的慢性拔毛癖的研究中,作者使用了反应中断(作者将其称为反应校正),其中包括治疗师将女性的手放在她身边或放在她的腿上 5 秒。关于头发拉扯或操纵的事件(Maguire 等人,1995 年)。这个程序类似于其他研究中使用的那些以身体为中心的重复行为,例如自伤手嘴(Rapp et al. 2000a, b; Turner et al. 1996)。尽管响应中断程序减少了行为,但 Maguire 等人。 (1995)表明,使用反应预防的干预,根据目标行为的发生情况将手套戴在女性的手上,比反应中断程序更成功。在文献中,反应中断、重定向或预防通常与其他程序相结合,例如差异强化(例如,McEntee 等人 1996;Rapp 等人 2000a,b)。拉普等人。 (2000a, b) 实施了响应中断 (RI) 和差异强化 (DRO)
手腕负重和非偶然使用手套后的智障女性在几次训练中未能减少她的头发拉扯和头发操作。反应中断涉及治疗师将参与者的手臂在她身边保持 20 秒,这取决于拉头发。差异强化涉及治疗师称赞参与者没有拉扯头发
重置间隔计划,从 30 秒逐渐增加到 10 分钟。 RI 和 DRO 干预立即将头发拉扯和头发操作降低到零或接近零的水平。此外,当参与者的母亲在家中实施干预时,治疗效果持续了几个疗程并保持。文献中的研究结果表明,包括反应中断、反应重定向、反应预防和差异强化的某种组合的多组分干预措施对于减少以身体为中心的重复行为是有效的。然而,缺乏评估单个治疗成分的成分分析导致不确定任何一种程序作为以身体为中心的重复行为的治疗方法的效用。我们认为,在转向需要更多努力和时间来实施的多成分干预措施之前,可能需要对其中一个单独的治疗成分(例如反应中断或重定向)进行初步评估。如果单个治疗成分被证明有效,则可以避免额外的程序,如果证明无效,则可以添加额外的程序。
惩罚惩罚的特点是当行为发生特定后果时行为的减少(Miltenberger 2016)。惩罚的两种变体包括积极惩罚,其中在行为之后呈现厌恶刺激,或消极惩罚,其中在行为之后移除强化刺激(Miltenberger 2016)。各种形式的惩罚已被用于减少 IDD 患者以身体为中心的重复行为(例如,Altman 等人 1978;Barmann 和 Vitali 1982;Barrett 和 Shapiro 1980;Corte 等人 1971;Gross 等人 1982)。一种用于减少以身体为中心的重复行为的惩罚形式是面部筛查。面部筛查利用围兜的简短应用来覆盖个人的面部,具体取决于问题行为。 Barmann 和 Vitali (1982) 评估了面部筛查在治疗三名智障儿童拔毛时的有效性。在干预中使用围兜并没有限制儿童的呼吸,并且被认为是护理人员可以接受且符合伦理的干预措施。结果表明,面部筛查程序将所有三个孩子的头发拉扯减少到零。此外,拉毛在几个月内保持在零
为所有三个孩子,并为在校的两个孩子保持在额外的学校环境中。其中两个孩子的父母报告还表明,之前因拔毛造成的组织损伤和秃斑已经痊愈。因为它涉及刺激的反应-条件呈现和随后的行为减少,面部筛查将被视为一种形式
正面惩罚。过度矫正是另一种形式的积极惩罚,用于减少以身体为中心的重复行为。在过度校正过程中,会根据问题的发生提示做出努力的响应
行为(Miltenberger 2016)。在关于 IDD 个体表现出的以身体为中心的重复行为的文献中,过度矫正的成功例子包括口腔卫生程序,包括使用消毒液刷牙和牙龈以用于慢性手口(Foxx 和 Azrin 1973)和用于拔毛的刷毛程序(巴雷特和夏皮罗 1980 年)。因为矫枉过正
需要与不良行为的地形或行为对环境的影响相关的努力响应,它可能被视为一种可接受的惩罚形式。其他针对以身体为中心的重复行为的积极惩罚程序,例如偶然的芳香氨和电击(Altman et al. 1978; Corte et al. 1971),可能不被认为是可接受的。
虽然 Corte 等人。 (1971 年)表明,偶然电击消除了 IDD 个体中以身体为中心的自我伤害性重复行为,电击通常被视为一种不可接受甚至不道德的程序,因此不太可能在当代实践中使用(Miltenberger 等人,1989 年)。奥特曼等人。 (1978) 使用或有芳香氨来减少脑瘫年轻女孩的头发拉扯和中度智力残疾的年轻男孩咬手指的情况。该程序涉及在参与者的 n 附近挥动一个打开的氨胶囊ose 取决于问题行为。奥特曼等人。发现该程序在应用 3 秒时可有效减少小女孩的头发在多个设置中拉扯,并在应用 1 秒时减少小男孩的手指咬伤。这些结果表明,不同时间的或有氨暴露可能有效减少以身体为中心的重复行为。然而,类似于使用休克作为干预措施,芳香氨的使用在当代实践中可能被认为是不可接受的。如果甚至考虑过,这种程序的使用将被保留用于危险且难以处理的以身体为中心的重复行为。与用于治疗以身体为中心的重复行为的其他干预措施类似,惩罚已与其他程序(例如差异强化)结合使用(Altman 等人 1978;Gross 等人 1982)。例如,格罗斯等人。 (1982 年)评估了两种联合干预措施对脑瘫和智力残疾小男孩拉头发的影响。这些干预措施是过度矫正和面部筛查,每一项都与其他行为的差异强化 (DRO) 相结合。在这两个程序中,每 10 秒的时间段都会给予表扬,并且没有拉扯头发的情况。在 DRO 和过度矫正过程中,治疗师将男孩的手臂举过头顶并在身体前面持续 2 分钟,具体取决于每次发生
头发拉。在 DRO 和面部筛查过程中,根据每次拉扯头发的情况,将围兜放在男孩的脸上 15 秒。格罗斯等人。发现这两种干预措施都减少了参与者的头发拉扯,但面部筛查程序更有效。此外,随着拉毛减少到接近于零,孩子玩得更合适,参与的学术活动也更多。此外,拔毛引起的组织损伤在 6 周的随访期内愈合。
如果没有成分分析,则只能推断使用组合程序的研究中的关键治疗成分。在治疗特别有害或威胁健康的行为过度时,例如
导致严重组织损伤的以身体为中心的重复性行为,通常尽可能有效和高效地治疗行为符合客户的最大利益,这可能取代评估单个治疗成分的需要。因此,这些研究的结果证明了有效的治疗方法,但并未证明一种成分与行为减少之间的功能关系。
意识增强装置
意识增强装置 (AED) 是由 Rapp 等人设计的电子设备。 (1998)发出的音调取决于一个人的手靠近一个人的头部。一位智障女性表现出的习惯逆转未能减少头发拉扯和头发操作导致了 AED 的发展。
AED 的目的是提高对她的目标行为发生的认识,促使使用竞争反应(将她的双臂交叉放在胸前),并提供一种厌恶的听觉刺激,起到积极的惩罚作用。当 AED 的声音响起时,这位女士被教导要使用她的竞争反应来拉扯头发。 AED 发出视她而定的音调
手在她头部 6 英寸的范围内移动。当 AED 启动时,女性的头发拉动和操作立即减少到接近零,随后保持在零或接近零的水平。其他研究已经证明了使用 AED 与拇指吮吸(Stricker 等人,2001 年)和手指吮吸(Ellingson 等人,2000 年)的类似效果。一项研究使用 AED 来减少被诊断患有注意力缺陷障碍的年轻女孩的手指吸吮,并发现单独使用 AED 并不能消除手指吸吮(Stricker 等人,2003 年)。然而,在 AED 中增加了一个遥控蜂鸣器,蜂鸣器分贝水平的增加立即降低了
在治疗后的几周内,手指吸吮为零并保持零或接近零水平。如图 6.3 所示,在基线和儿童佩戴 AED 未激活的阶段(非激活 AED)之后,使用 AED 并没有降低行为(激活 AED)。一旦添加了额外的蜂鸣器(主动 AED 启动),手指吸吮减少到低水平。
顾名思义,AED 发出的音调增强了目标行为发生时的意识。如果参与者已经学会了竞争响应,则音调可以提示使用竞争响应。 AED 发出的音调也可能对行为的前兆运动起到积极的惩罚作用,使习惯行为不太可能发生。此外,移动
离开头部的手可能会因音调的终止而受到负面加强(Rapp et al. 1998)。无论其功能如何,AED 似乎都是一种有效的治疗方法,可以减少以身体为中心的威胁健康的重复行为,并为智障人士带来希望。希姆勒等人。 (2008) 认为意识到习惯行为的前兆运动,
习惯行为可能发生的情况,以及习惯行为的功能是成功逆转习惯所必需的。这种对意识重要性的强调可能是对智障人士改变习惯无效的一种解释。此外,它表明自动干预,例如不需要行为意识的 AED,或实施竞争反应所需的技能集,或护理人员的存在以实施突发事件,可能是理想的身体干预措施。 IDD 患者表现出的集中重复行为。更多的
有必要进行研究,以确定 AED 作为独立程序的有效性和普遍性,并作为 IDD 患者习惯逆转的辅助手段。实践建议 到目前为止,我们已经描述了五种基于证据的实践,这些实践已用于治疗智障人士以身体为中心的重复行为:习惯逆转、差异强化、反应中断、重定向或预防、惩罚和意识增强装置.这些干预措施已被证明在一定程度上有效减少或消除该人群以身体为中心的重复行为。本节将回顾
这些干预措施并为临床实践中的治疗选择提供建议。
习惯逆转是对非残疾个体的神经习惯和抽动最有效的治疗方法之一(Miltenberger et al. 1998a, b; Woods and Miltenberger 1995)。习惯逆转有助于提高对不良行为的认识,并使用竞争性反应来替代不良行为(Azrin 和 Nunn 1973)。不幸的是,研究表明习惯逆转并不是
通常对 IDD 患者有效(例如,Rapp 等人 1998)。习惯性逆转对 IDD 患者的效果有限,这可能是由于自然环境中缺乏使用竞争反应的强化、缺乏减少习惯行为的动力或难以意识到不良行为(Long et al. 1999)。习惯逆转可能会成功减少
以身体为中心的重复行为,如果客户有动机改变他或她的行为并受到行为的社会后果的影响。改变的动机很可能是行为带来的不便、耻辱或不愉快的社会后果的产物。如果患有 IDD 的客户没有经历这些事件或不受这些事件的影响,则客户不太可能有动力去改变
行为,因为减少行为不会起到 r 的作用强化剂。龙等人。 (1999 年)发现,对于被诊断患有轻度智力障碍的男性,由于咬指甲而对自己的指甲外观表示不满,这种习惯逆转最为成功。这名男子还报告了以前自发尝试停止咬指甲。尽管额外的意外情况
需要消除他的指甲咬伤,习惯逆转减少了他从事这种行为的时间。如果来访者表达了停止其习惯行为的动机,则在临床环境中利用习惯逆转可能是有益的。
在适当的时候,习惯逆转是一种可取的干预,因为一旦学会了竞争反应,客户就可以在他或她的自然环境中实施竞争反应,而无需治疗师或护理人员的外部突发事件。习惯逆转可能会促进功能独立,这符合接受治疗的个人的最大利益。然而,还需要更多的研究来
确定何时改变习惯可能对智障人士有效,以及哪些辅助程序可以提高其有效性。差异强化已在几项研究中用于治疗 IDD 患者的以身体为中心的重复行为(例如,Cavalari 等人,2013;
考德里等人。 1990;朗等人。 2009;拉德斯塔克等人。 2011;拉普等人。 2000a, b;罗斯科等人。 2013)。它已单独使用,也可与其他干预措施(如习惯逆转)结合使用。差异强化可以采用不同的形式,包括 DRA、DRI 或 DRO。差异强化也可以针对与行为相关的特定用途进行修改,例如
用于咬手指的客户的指甲生长(例如,Long et al. 1999)。
差异强化使用正强化的原理来增加期望的行为和消退以减少不期望的行为。差异强化是一种有效且可接受的治疗方法。此外,还有
通过选择期望行为的强化物以及选择要强化的替代或不相容行为,将客户的偏好和选择纳入治疗的机会(Radstaake et al. 2011)。
在开发将推广到客户自然环境的干预措施时,需要考虑客户的偏好和选择。尽管差异强化有几个优点,但一个缺点可能是难以实施。差异化强化通常需要其他负责观察客户的人实施,根据期望行为的发生或目标行为的不发生提供适当的强化物,并根据目标行为的发生拒绝强化物。对于实施干预的人来说,监测要求可能涉及不可接受的高水平响应工作,这一点很重要,尤其是当治疗必须
由家长、教师或工作人员实施。自我监控和自我管理的差异强化可能是传统差异强化程序的可行替代方案;然而,需要更多的研究来确定它是否对不同程度的智障人士有效。反应中断、重定向和预防是干预措施,包括在序列的早期中断行为,重定向到所需的替代行为,并通过在身体上施加物理约束或障碍来防止不良行为。这些方法已单独使用,并与差异强化相结合,以减少以身体为中心的重复行为,例如用手咬、拉头发和操纵头发。尽管没有考虑解决行为强化后果的功能性干预,但如果反应预防掩盖了强化后果,则它可能是功能性的。
如果客户被指示操纵与重复行为产生的刺激相匹配的刺激,则由行为和反应重定向引起的刺激可能是有效的(例如,Rapp et al. 1999) 只有一项研究直接解决了身体的自动强化功能- 通过使用乳胶手套来掩盖刺激的集中重复行为(拉头发)
(图 6.2)并为客户提供与拉毛产生的刺激相匹配的刺激(Rapp et al. 1999)。图 6.2 显示了提供匹配刺激对头发拉动和头发操作的影响。当客户有“自由头发”时,她不再拉她的头发并操纵自由头发,而不是拉头发并操纵它。在使用差异强化时,与持续监控客户行为的要求相关的困难也出现了有回应
中断和重定向,实现者必须持续观察客户端,以便在行为发生时中断和重定向。这种困难可能会对使用以身体为中心的重复行为的响应中断和重定向造成不利影响。但是,以将手套或夹板戴在参与手的客户的手上的形式进行响应预防
嘴巴或头发拉扯通过简单的障碍或在某些情况下通过解决感觉刺激功能来减少行为。此外,由于它不需要社交调解,因此它是一个可以在工作人员时使用的程序
不能持续与客户在一起或当客户独自一人时(Deaver et al. 2001; Rapp et al. 2000a, b)。应与护理人员讨论手套或手夹板等反应预防装置的使用(以及任何干预措施),以确定该程序的可接受性。此外,应制定治疗褪色计划,以消除屏障的使用
设备。另一种不需要实施者与客户一起持续存在于环境中的干预措施是意识增强设备 (AED)。如前所述,AED 是一种发出声音的电子设备
当佩戴者将手移向他或她的头部时(它也可以被编程为包括其他身体部位或位置)。少数评估 AED 有效性的研究的结果表明,它可以减少以身体为中心的
智障人士的重复行为,包括拉头发和吮吸拇指(Rapp 等人 1998;Stricker 等人 2001)。 AED 促进获得替代行为,通过终止蜂鸣器来负面加强,同时通过积极惩罚减少不受欢迎的行为,而无需护理人员或工作人员在场监控行为
并实施干预(Rapp et al. 2000a, b)。 AED 是一种很有前途的干预措施,可以减少智障人士以身体为中心的重复行为。需要更多的研究来评估 AED 对多种威胁健康行为和不同残疾个体的影响。除了安排自动负强化和正惩罚意外事件外,AED 还增强了对产生语气的行为发生的认识。任何时候在干预中使用惩罚时,都必须注意确保个人能够获得替代的强化来源,并且相关人员可以接受治疗。用于治疗以身体为中心的重复行为的惩罚形式包括
面部筛查、过度矫正、电击和芳香氨(例如,Altman 等人 1978;Barmann 和 Vitali 1982;Barrett 和 Shapiro 1980;Corte 等人 1971;Gross 等人 1982)。尽管使用诸如电击等强烈惩罚形式的干预措施已被证明可有效减少自伤行为(Corte 等人 1971;Favell 等人 1982;Linscheid 等人 1990),但我们
不建议将这些方法用于以身体为中心的重复行为,因为它们的可接受性有限,并且在当代实践中侧重于功能性和非厌恶性方法。在可能的情况下,应使用积极的干预措施
在涉及惩罚的干预之前(Bailey 和 Burch 2011)。近年来,研究已经从惩罚程序转向积极干预,但需要更多的研究来确定积极干预是否同样有效,以及临床实践是否遵循研究趋势(Matson 和 LoVullo 2008)。 (Matson 和 LoVullo 2008)。
在确定针对以身体为中心的重复行为的治疗方法时,必须考虑几个因素,包括行为的严重程度和消费者的价值观。如果行为严重或危及生命,则可能有必要使用惩罚,如果它可以最有效地减少行为。如果积极的做法未能将威胁健康的行为降低到可接受的水平,惩罚也可能是干预的必要组成部分。然而,惩罚应始终与强化程序相结合,例如差异强化或非偶然强化(Lerman 和 Vorndran 2002)。与任何治疗选择过程一样,应考虑惩罚的利弊。例如,尽管在 Altman 等人的一项研究中,偶然的芳香氨在减少拉扯头发和咬手方面是有效的。 (1978 年),在实施过程中出现了几个问题,包括由于社会污名、环境挑战、不断变化的行为形态以及难以监测和识别行为发生而导致的管理困难。最终,我们不建议涉及应用程序的惩罚由于该领域的当前理念、有限的可接受性以及有效的、侵入性较小的程序的可用性,厌恶刺激的合理化。
从业者应评估其特定客户的需求,并根据关注的行为、消费者的价值观、道德准则和文献中的经验支持确定最佳方案。



















 被折叠的 条评论
为什么被折叠?
被折叠的 条评论
为什么被折叠?
 到【灌水乐园】发言
到【灌水乐园】发言











