





肯尼亚第三方支付
COVID-19 cases in Kenya are accelerating rapidly. New cases have increased 300% month-over-month since April of this year while global and regional media have reported on the economic toll of stringent lock-down measures and heavy-handed government practices.
肯尼亚的COVID-19病例正在Swift增加。 自今年4 月以来, 新案件数量环比增长了300% ,而全球和区域媒体都报道了严格的封锁措施和严厉的政府做法 造成的经济损失 。
In previous posts, we explored how Africa and the rest of the world have struggled to understand the full extent of the pandemic on the continent. To date, there is no comprehensive analysis of how the crisis is playing out in sub-Saharan Africa and until now, the global community has been guilty of using limited data (cases and deaths) in most analyses, presenting a lopsided and incomplete picture of the pandemic in Africa.
在以前的文章中,我们探讨了非洲和世界其他国家如何努力了解该大陆的整个流行病范围。 迄今为止,尚无关于撒哈拉以南非洲危机如何蔓延的全面分析,直到现在,全球社会一直在大多数分析中使用有限的数据(案件和死亡),这使该组织歪曲而又不完整。非洲大流行。
To address this gap we have developed a bespoke analysis that integrates typical epidemiological datasets with population mobility data from Google Mobility reports and policy data from Oxford. We explore these data sources separately and in combination with one another through in an illustrative use case for Kenya. We then go a step further by comparing these data sources to a recent pre-print seroprevalence study, which adds deeper dimension to testing positivity and antibody presence in Kenyan populations.
为了解决这一差距,我们开发了定制分析,将典型的流行病学数据集与Google Mobility报告中的人口流动数据以及牛津大学的政策数据相集成。 在肯尼亚的一个示例性用例中,我们将分别或相互结合地探索这些数据源。 然后,我们通过将这些数据源与最近的印刷前血清阳性率研究进行比较 ,从而进一步走了一步,该研究为检测肯尼亚人群的阳性和抗体存在增加了更深的层面。
For the first part of this analysis, we used three publicly-available datasets to construct a composite snapshot of the COVID-19 pandemic within Kenya from February 10th — August 10th.
对于此分析的第一部分,我们使用了三个公开可用的数据集,构建了2月10日至8月10日肯尼亚境内COVID-19大流行的复合快照。
Comparing these data side by side, we found the following:
并排比较这些数据,我们发现:
1.政府政策只在短时间内限制了日常活动,肯尼亚人继续上班 (1. Government policies only restricted daily movements for a short time and Kenyans continued to go to work)
When restrictions (e.g. public events, gatherings, educational institutions) were implemented in early March, data showed a decline in mobility to grocery stores and pharmacies, parks, retail and transit stations.
3月初实施限制措施(例如公共活动,聚会,教育机构)时,数据显示,前往杂货店和药房,公园,零售和公交车站的出行人数有所减少。
In June, there was a gradual return to baseline mobility while many restrictions were still in place. Comparable rise in mobility for residences is not observed around the same period (early March). Instead, the rise in mobility for places of residence is much more gradual. This may be due to non-residence locations (grocery stores, parks, etc.) being easier to identify using mobile phone data compared to an individual’s “home.”
6月份,基线流动性逐渐恢复,但仍存在许多限制。 在同一时期(3月上旬),没有观察到居民流动性的可比增长。 取而代之的是,居住地流动性的增加是渐进的。 这可能是由于与个人的“家”相比,使用手机数据更容易识别非居住位置(杂货店,公园等)。
There is also a cyclical pattern for workplace mobility, indicating that many Kenyans were not working from home, likely because their job was not conducive to remote work. Another possible explanation is that, while the Kenyan government provided some financial relief, it may not have been sufficient to fully supplement Kenyans’ financial requirements.
还有一种周期性的工作场所流动模式,表明许多肯尼亚人不是在家工作,可能是因为他们的工作不利于远程工作。 另一个可能的解释是, 虽然肯尼亚政府提供了一些财政救济, 但可能不足以 完全补充肯尼亚人的财政需求。
2. 每天新发病例和死亡人数Swift增加,但化验数量也在增加 (2. Daily new cases and deaths are rapidly rising — but so are the number of tests)
Throughout March and April, daily new cases in Kenya remained extremely low until approximately mid- to late-May when they began to rise. COVID-19 deaths were also generally low until June when they began to rise. Notably, up until June, 60% of days did not have a single COVID death, but since June 1st, there has not been a single day without a COVID-19 death and August is seeing average daily deaths in the double digits.
在整个3月和4月,肯尼亚的每日新病例一直保持极低的水平,直到大约5月中下旬才开始上升。 直到6月开始上升之前,COVID-19的死亡人数也普遍较低。 值得注意的是,到6月为止,有60%的日子没有发生过一次COVID死亡, 但是自6月1日以来,没有一天没有发生过COVID-19死亡,而8月的平均每日死亡人数达到了两位数。
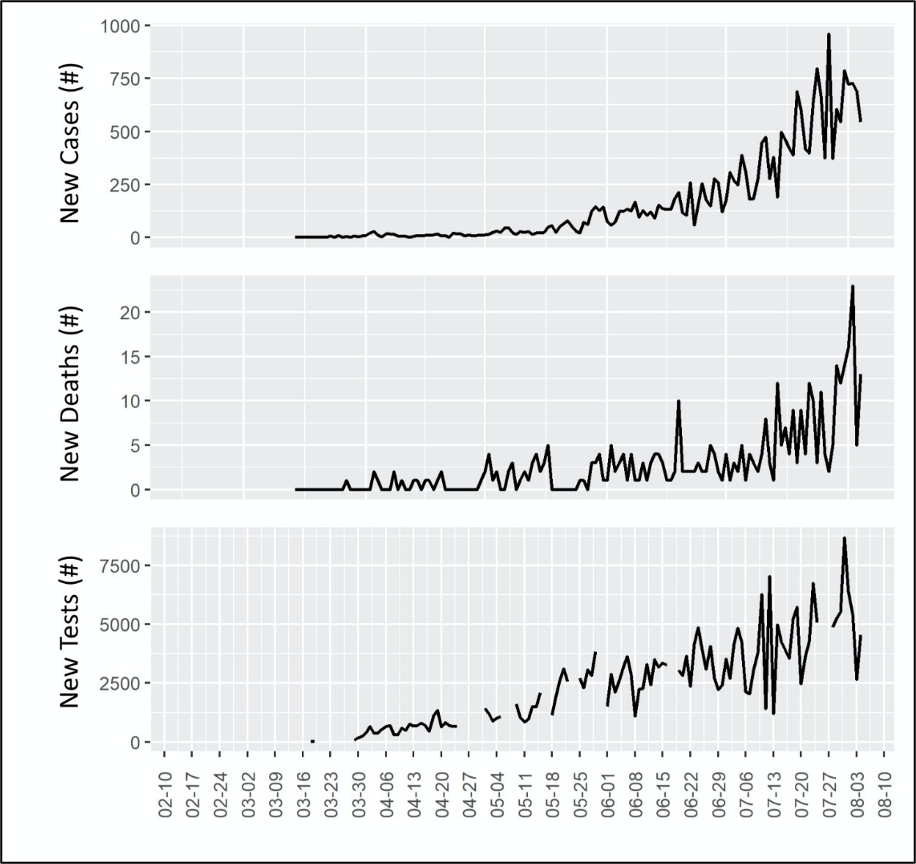
What, however, was the testing capacity was during this time period and how could it have changed over the past few months? We see that the pattern of new daily COVID-19 tests follows a very similar pattern to that of both cases and deaths. While there is some missing testing data in the early months, there is a clear association between increasing case and death detection and tests done.
但是,这段时间内的测试容量是多少?过去几个月中它有什么变化? 我们看到,每天进行新的COVID-19测试的模式与病例和死亡的模式非常相似。 尽管在最初的几个月中缺少一些测试数据,但是在增加的病例和死亡检测与完成的测试之间存在明显的关联。
3.尽管肯尼亚政府最初实施了严格的政策,但短暂的平静之后,案件继续增加 (3. Despite stringent policies initially implemented by the Kenyan government, after a short lull, cases continue to rise)
Another critical insight for understanding a nation’s COVID-19 response is the policy landscape. The Oxford COVID-19 Government Response Tracker systematically collects, analyzes and presents policy responses over time, in countries around the globe, across several indicators.
了解一个国家对COVID-19的回应的另一个重要见解是政策格局。 牛津COVID-19政府React跟踪器在全球范围内跨多个指标系统地收集,分析并提出了随时间推移的政策React。
From these data, we can see that public information campaigns were the first policy tool implemented in Kenya in February, suggesting that the government acknowledged the threat of COVID-19 early on. The next wave of policies came into play on March 14th — the date of Kenya’s first confirmed COVID case. On that date, we see sweeping regulations on international travel, public events, gatherings, workplaces, and schools.
从这些数据中,我们可以看到,公共宣传运动是2月份在肯尼亚实施的第一个政策工具,这表明政府早就意识到了COVID-19的威胁。 新一轮政策于3月14日生效-肯尼亚首例确诊的COVID案发生之日。 那天,我们看到了有关国际旅行,公共活动,聚会,工作场所和学校的全面法规。
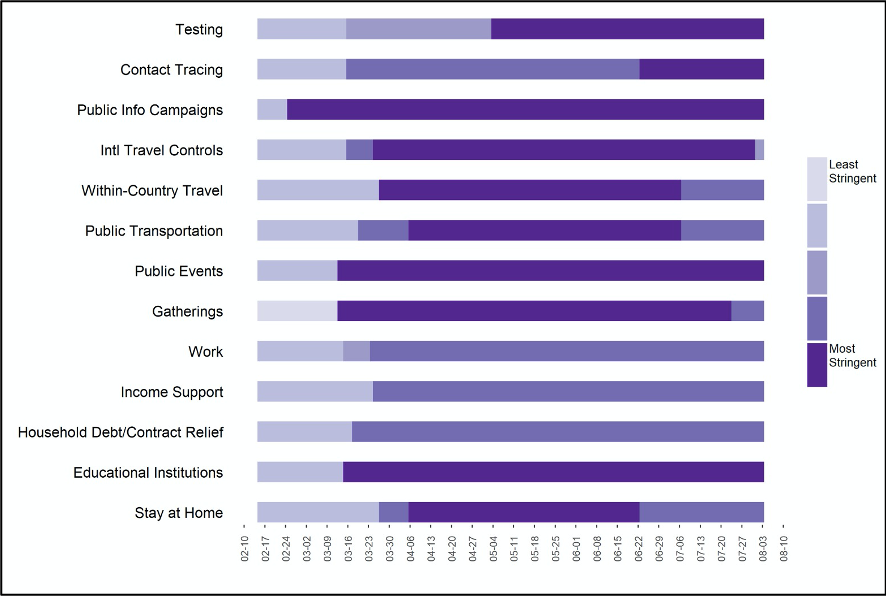
Viewing policy data compared against testing data, we see that more liberal testing policies were put in place the first week of May. In April, the average number of new daily tests was about 650 and after testing policy expanded, average new tests in May tripled to nearly 1,900. We can see an additional surge in new daily tests from June to July when contact tracing policies intensified, resulting in an increase from 3,000 to 4,300 new tests per day on average.
查看政策数据与测试数据的比较,我们发现5月第一周实施了更为宽松的测试政策。 4月份,平均每日新测试次数约为650次,并且随着测试政策的扩大,5月份的平均新测试次数增加了两倍,达到近1900次。 从6月到7月,随着接触追踪政策的加强,我们发现新的日常测试会进一步激增,平均每天新测试从3,000个增加到4,300个。
Finally, we draw attention to the stay-at-home policy, gradually enacted in late March with a full lockdown in place by early April — lasting through June 22nd. From Google Mobility data, this policy coincides with a nearly 50% reduction in mobility during roughly the same time period. Notably however, mobility began to decline well ahead of a stay-at-home order and began returning to normal levels before the lockdown was truly lifted. This indicates that public information campaigns and individual behaviors were critically important early in the epidemic, while the economic demand to return to work and normal life activities led to more mobility in June and July — despite policies recommending otherwise.
最后,我们提请注意“在家办公”政策,该政策于3月下旬逐步颁布,并在4月初(到6月22日)全面锁定。 根据Google Mobility数据,此政策与大致在同一时间段内的移动性降低了近50%相吻合。 但是,值得注意的是,在居家订购之前,流动性开始大大下降,并在真正解除锁定之前开始恢复到正常水平。 这表明,在流行病初期,开展公共宣传活动和个人行为至关重要,而在经济方面,恢复工作和正常生活活动的需求在6月和7月导致了更多的流动性,尽管政策另有建议。
4.一项新的血清阳性率研究显示SARS-CoV-02抗体水平升高 (4. A new seroprevalence study shows rising levels of SARS-CoV-02 antibodies)
Despite available data on mobility, new cases, deaths, tests and policy, understanding the true underlying epidemiology of COVID-19 remains elusive given severe limitations in testing and potential biases arising from who gets tested, has severe disease and dies.
尽管有关于流动性,新病例,死亡,检测和政策的可用数据,但鉴于检测的严重局限性以及由于接受检测的人,患有严重疾病和死亡的潜在偏见,对COVID-19真正的潜在流行病学的了解仍然难以捉摸。
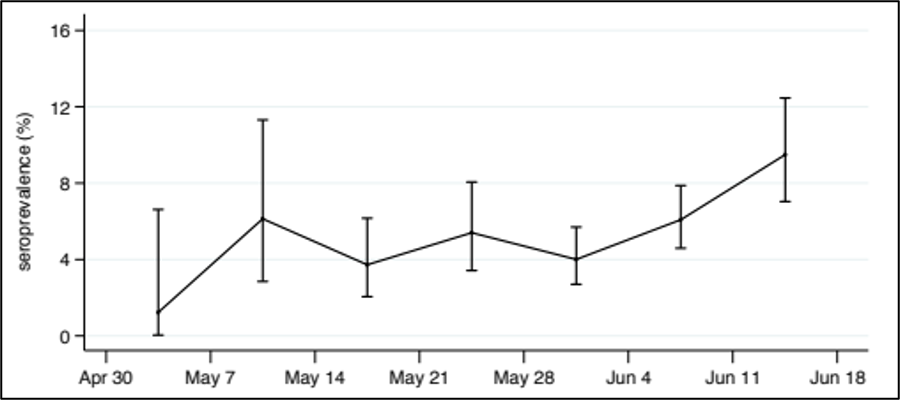
New data from a preprint (not yet peer reviewed) study on the seroprevalence of anti-SARS-CoV-2 IgG antibodies in Kenyan blood donors may provide clues as to the true trends of incidence and prevalence of COVID-19 in Kenya.
预印本(尚未经过同行评审)研究中 的抗SARS-CoV-2 IgG抗体血清阳性率的 新数据 肯尼亚的献血者 可能提供有关肯尼亚COVID-19发生率和患病率真实趋势的线索。
A seroprevalence study uses serology tests to identify people in a population that have antibodies against an infectious disease in order to estimate the percentage of the population that may have been infected. In addition, it shows how an infection progresses through the population over time.
血清阳性率研究使用血清学检测来鉴定人群中具有抗传染病抗体的人群,以估计可能已感染人群的百分比。 此外,它还显示了随着时间的推移,感染如何在整个人群中发展。
In Kenya, the study population’s seroprevalence hovered around 5% throughout May and has been slowly rising since early June.
在肯尼亚,整个五月份,研究人群的血清阳性率徘徊在5%左右,自六月初以来一直在缓慢上升。
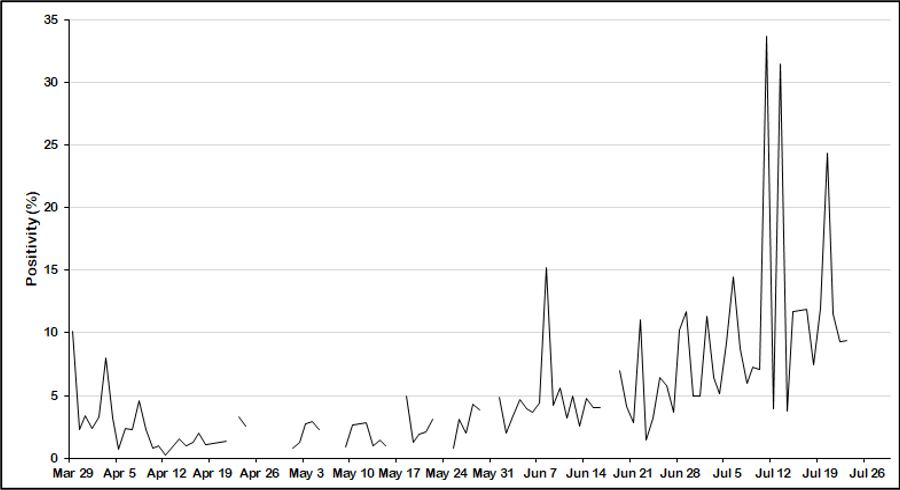
Similarly, Kenya’s test positivity rate — the percentage of all tests conducted that come back positive — was also increasing in early June. The test positivity rate remained below 10% until early June and increased dramatically in early July.
同样,肯尼亚的考试阳性率(所进行的所有考试中恢复阳性的百分比)在6月初也有所增加。 直到6月初,测试阳性率仍低于10%,7月初急剧上升。
Combining our four data sources including the seroprevalence data indicates that COVID-19 incidence has been rising in Kenya as early as May. However, stay-at-home orders were not lifted until the end of June. So why did COVID-19 begin spreading so early and so rapidly?
结合我们的四个数据来源(包括血清阳性率数据),表明肯尼亚最早5月份的COVID-19发病率一直在上升。 但是,直到6月底才取消了全屋服务订单。 那么,为什么COVID-19这么早又如此Swift地开始传播?
1. 待在家里的命令和禁止社交聚会会影响出行能力,但个人行为也会造成影响 (1. Stay-at-home orders and bans on social gatherings have an impact on mobility — but so do individual behaviors)
Stay-at-home orders and restrictions on social events and gatherings likely had a significant impact on population mobility. There was also a clear return to more normal mobility before lockdown was lifted and even while social distancing recommendations remained in place.
留在家里的订单以及对社交活动和聚会的限制可能会对人口流动产生重大影响。 在解除锁定之前,甚至在保持疏远社交的建议仍然存在的情况下,也明显恢复了正常的出行。
The likely explanation is that people needed to meet their subsistence and household income needs and economic support from the government wasn’t enough. To sustain individual behavior change over periods longer than a month, nations must provide adequate and effective economic and psychosocial support if maintaining limited contact is a priority.
可能的解释是,人们需要满足他们的生活和家庭收入需求,而政府的经济支持还不够。 为了在一个多月的时间内维持个人行为的改变,如果必须优先保持有限的联系,各国必须提供充分有效的经济和社会心理支持。
2.政府的测试政策至关重要 (2. Government policies on testing are critically important)
The expansion of testing and contact tracing policies resulted in drastic increases in average daily testing levels, increasing capacity by thousands of tests per day.
测试和联系人跟踪策略的扩展导致平均每日测试水平急剧增加,每天增加了数千个测试的容量 。
This highlights the importance of government action in procuring commodities and supporting supply chains to ensure the availability of treatments, hospital supplies and infrastructure and personal protective equipment.
这突出了政府在采购商品和支持供应链以确保治疗,医院用品,基础设施和个人防护设备的可用性方面采取行动的重要性。
3.测试率和测试阳性率增加。 (3. Testing rates and test positivity increased.)
Although testing rates did increase dramatically over the time period, we also saw that test positivity increased, suggesting that the increase in tests alone did not account for the increase in cases.
尽管在此期间测试率确实显着增加,但我们也看到测试阳性率增加,这表明仅测试的增加并不能说明病例数的增加。
Along with the trending seroprevalence data, it is safe to assume that underlying incidence was (and is still) on the rise. Only by taking each data source into consideration simultaneously can we draw accurate conclusions about the epidemiology of COVID and inform policy accordingly.
连同趋势的血清流行率数据一起,可以安全地假设潜在的发病率正在(并且仍在)上升。 只有同时考虑每个数据源,我们才能得出关于COVID流行病学的准确结论,并相应地告知政策。
Overall, we saw that increased mobility, despite stringent country policies or increased testing, is likely the primary reason for the increase of COVID cases in Kenya. Renewed focus on policies which mitigate economic and psychosocial harm, while enabling responsible and safe behavior, will be key to sustaining a long-term response to the crisis.
总体而言,我们看到,尽管采取了严格的国家政策或加大了测试力度,但流动性的增加可能是肯尼亚COVID病例增加的主要原因。 重新关注减轻经济和社会心理伤害的政策,同时实现负责任和安全的行为,将是维持长期应对危机的关键。
肯尼亚接下来要做什么? (What’s next for Kenya?)
Our goal with this analysis was to identify underlying epidemic patterns from atypical combinations of publicly available data sources. In doing so, we reveal a data-driven, multidimensional view of Kenya’s experience with the COVID-19 pandemic.
我们进行此分析的目的是从可公开获得的数据源的非典型组合中识别潜在的流行病模式。 通过这样做,我们揭示了肯尼亚在COVID-19大流行中的经验的数据驱动的多维视图。
As a global community, we have a mandate to think of fresh questions, hypothesize answers and generate new leads that may help slow or stop the ongoing crisis. In a previous post, we outlined a balanced approach that may offer another way to slow the spread of COVID-19 across the African continent.
作为一个全球社区,我们负有思考新问题,假设答案并产生新线索的任务,这可能有助于减缓或阻止持续的危机。 在上一篇文章中,我们概述了一种平衡的方法 ,它可能提供另一种方法来减缓COVID-19在非洲大陆的扩散。
Kenya could benefit from implementing hyper-targeted, data-driven strategies that take into account their population’s response to top-down policies. Knowing the location and frequency of population movement, combined with regular review of seroprevalence rates and typical testing data, could lead to clearer informational campaigns, informed placement of testing sites or public-safety strategies in key areas.
肯尼亚可以从实施针对性强,数据驱动的战略中受益,这些战略考虑了其人口对自上而下政策的React。 了解人口流动的地点和频率,并定期检查血清阳性率和典型的检测数据,可以导致开展更清晰的信息运动,知情的检测地点布置或关键地区的公共安全策略。
Data is our most powerful tool against COVID-19. By leveraging its data, Kenya can implement better and more proactive policies and strategies to gain an edge against the pandemic.
数据是我们针对COVID-19的最强大工具。 通过利用其数据,肯尼亚可以实施更好,更主动的政策和策略,以取得对抗大流行的优势。
This analysis was led by Cooper/Smith’s resident interns Nathali Gunawardena and Deborah Chan, Masters of Science in Public Health students at McGill University and supervised by Dylan Green, MPH, PhC in Epidemiology at University of Washington. Nathali holds a BS in Biomedical Science with a minor in Psychology with extensive research experience on maternal and child health in Africa. Deborah is joint researcher and clinician as a Nurse with quantitative research interests in global health. Together, they have been invaluable members of our team as we continue to attempt to make sense of clinical and epidemiological data during the COVID-19 pandemic.
这项分析是由Cooper / Smith的常住实习生Nathali Gunawardena和Deborah Chan(麦吉尔大学的公共卫生专业硕士)以及华盛顿大学流行病学博士学位的Dylan Green指导的。 纳塔利(Nathali)持有生物医学科学学士学位,辅修心理学,在非洲的母婴健康方面拥有丰富的研究经验。 Deborah是一名联合研究员和临床医生,是一名护士,在全球卫生领域拥有定量研究兴趣。 他们在一起一直是我们团队的宝贵成员,因为我们继续尝试在COVID-19大流行期间理解临床和流行病学数据。
肯尼亚第三方支付















 1688
1688











 被折叠的 条评论
为什么被折叠?
被折叠的 条评论
为什么被折叠?
 到【灌水乐园】发言
到【灌水乐园】发言









