







❝日更149天
Lotus周六,周日,周一更新放射学前沿
全文字数10901字,阅读需要10min,建议收藏。
由于工作原因,需要做一份关于心脏的科研PPT,
正好发现了一篇2023年发表在Radiology上的文章

在上一期的文章中Lotus为大家进行了心肌细胞外容积分数(extracellular volume fraction,ECV)的基础介绍,
本期我们来对ECV的相关科研文章进行解读。
CT-ECV回顾
首先先带着各位朋友复习一下上节课的内容,还记得的朋友请自动跳到第二节。
虽然传统上使用心脏 MRI 进行无创采集,但心脏 CT-ECV是一种新兴的应用。
碘化造影剂是一种细胞外造影剂,弥漫性心肌纤维化和淀粉样沉积都会增加细胞外心肌空间,导致异常心肌中碘化造影剂的浓度升高。

在ECV的计算上,对于单能量 CT,
使用两次扫描前的 Hounsfield 单位(∆HU)差值用于评估造影剂的分布,以完成ECV-CT的计算,ECV-CT计算公式如下:
基于能量CT采集模式的 CT-ECV利用平衡期的碘图即可完成计算,因而可以减少钙化积分(平扫)这期扫描,大大地简化了扫描流程。
在能量成像采集中,ECV-CT 的计算公式为:
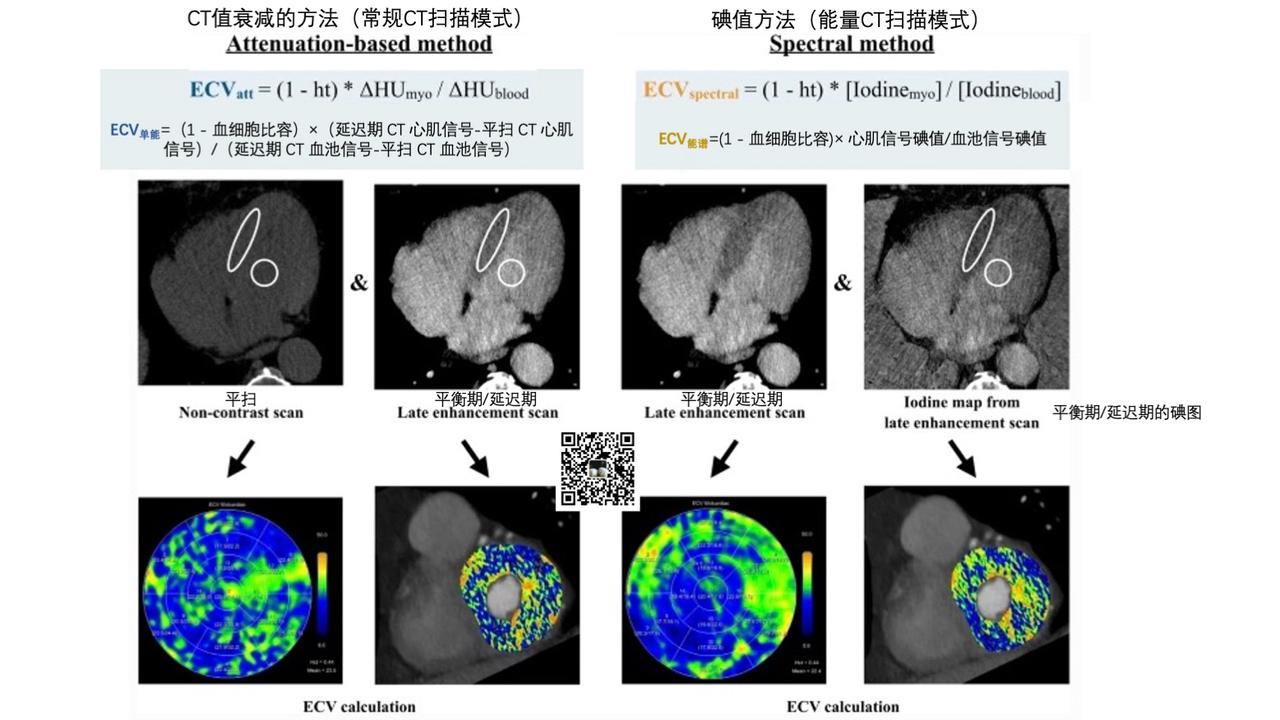
在ROI的勾画上,
手动勾画的话,
血池值的获得通常是在左心室腔内绘制感兴趣区 (region of interest,ROI),心肌内的感兴趣区通常勾画在室间隔位置。
随着技术的不断进步,
当代的 CT 软件可以生成半自动或全自动的整个心脏的 CT-ECV 图,
甚至目前出现了基于血管内CT衰减值自动合成血细胞比容的算法工具。
【Lotus:讲完所有的会出一个番外篇讲ECV的算法】
在扫描方案上:
-
延迟期扫描通常采用 与平扫相同的采集参数。 -
绝大多数研究采用了较晚时间点的,造影剂注射后 7min采集的心脏CT扫描方案。 -
根据目前的文献, 50-100 mL的固定用量或 1.4-1.8 mL/kg的较高浓度的造影剂用量似乎能为 ECV 计算提供足够的图像质量。
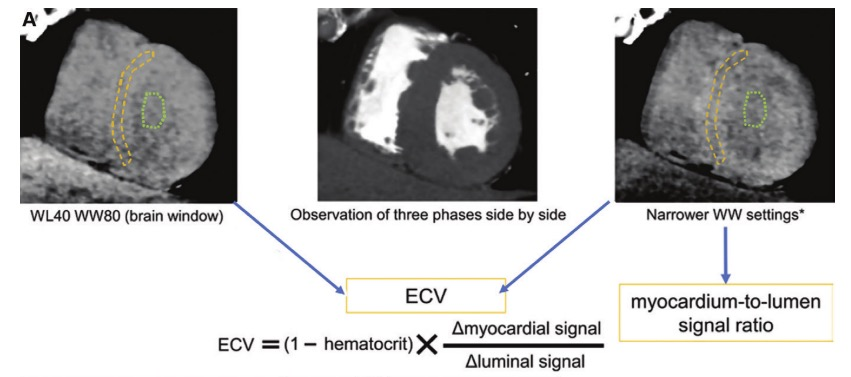
通常来说疾病造成的增加细胞外心肌空间表现为CT-ECV的升高:
如上左图为正常的心肌,
可以看到心肌CT衰减信号(75HU)小于血管/血池CT衰减信号(109.1HU),
计算得到的CT-ECV为23%。
如上右图为一野生型甲状腺素运载蛋白的心力衰竭患者,
可以看到心肌CT衰减信号(141.1 HU)大于血管/血池CT衰减信号(131.0 HU),
计算得到的CT-ECV为68%。
绿色箭头显示右心室壁出现的平衡期的异常增强,提示右心室淀粉样蛋白浸润。
CT-ECV的研究
心肌 ECV 可评估弥漫性心肌纤维化和浸润性心肌病的存在和程度,是缺血性和非缺血性心肌病的独立预后指标
CT-ECV 的可行性和临床实用性已在多种心血管疾病中得到证实:
| 作者 | 年 | 研究对象 | 病例数 | CT扫描 | 主要发现 | Ref |
|---|---|---|---|---|---|---|
| Ohta et al | 2020 | 心衰患者 | 79例 | 双能CT | 331 个节段的CT-ECV 和 MR-ECV 的平均值分别为 31.6 ± 9.1% 和 33.2 ± 9.1%。每个区域的 CT-ECV 和 MR-ECV 之间都有很强的相关性,具体如下:所有节段,r = 0.837;室间隔,r = 0.871;室间隔中部,r = 0.895;前部,r = 0.869;下部,r = 0.793;外侧,0.864(所有 p <0.001)。 | 53 |
| Abadia et al | 2020 | 缺血性和非缺血性心肌病 | 60例患者,10例对照 | 双能量CT | 健康心肌、非缺血性心肌病和缺血性心肌病的ECV中位数分别为25.4%、38.3%和36.9%; ECV >29.5%提示心肌病(敏感性90.3%,特异性90.3%)。 | 51 |
| Dubourg et al | 2021 | TAVR | 21 名重度主动脉瓣狭窄患者 | 双能CT | 与MR-ECV(29.1±3.9%)相比,CT-ECV(29.9±4.6 %略微高估了ECV(P<0.0001),按节段和按患者分析的偏差和一致性极限分别为+2.3%和+2.5%。 | 54 |
| Qi et al | 2021 | 心力衰竭(无CAD) | 60例患者,60例对照 | 双能CT | ECV是心力衰竭的独立风险因素(优势比为1.356,95%可信区间为[1.178-1.561]; P < .001); ECV与NT-proBNP、左室舒张末期容积、左室收缩末期容积、LAV均呈正相关(r分别为0.629、0.329、0.346和0.338;所有P <0.001)。 | 55 |
| Deux et al | 2021 | 心脏淀粉样变性患者 | 84例心脏淀粉样变性患者,43名非淀粉样蛋白性心脏肥大患者,33名对照组 | 常规CT | 心脏淀粉样变性患者的CT-ECV(平均值为54.7% ± 9.7%)高于非淀粉样蛋白性心脏肥大患者患者(平均值为34.6% ± 9.1%;P < .001)和无肥厚患者(平均值为35.9% ± 9.9%;P = .001)仅CT-ECV(危险比 >0.56 vs ≤0.56 = 4.2 [95% CI: 1.4, 11.8]))可预测心脏淀粉样变性患者的死亡率。 | 57 |
| Si-Mohamed et al | 2021 | 急性心肌炎 | 60例患者,18例对照 | 双能光子CT | 心肌炎患者的CT-ECV为31.60%,显著高于对照组(健康人)CT-ECV,AUC为0.835(P <0.001),敏感性和特异性分别为80%和78%。 | 65 |
| Yamasaki et al | 2021 | 接受肺动脉内膜切除术和/或球囊肺血管成形术治疗的患者(CPEPH) | 31例患者,8例对照 | 双能CT | CPEPH患者的ECV显著较低; CT-ECV与平均PAP、PVR和BNP之间存在显著相关性。 | 63 |
| Han et al | 2021 | TAVR | 109例主动脉瓣狭窄患者 | 双能CT | 接受TAVR的重度主动脉瓣狭窄患者中,LVEF恢复的患者的CT-ECV显著低于LVEF未恢复的患者(分别为29.4%和33.2%; P = 0.009)。在多变量分析中,主动脉瓣平均跨瓣压差、左心室舒张末期容积和ECV是LVEF早期恢复的独立预测因素。 | 85 |
| Suzuki et al | 2021 | TAVR | 95例接受TAVR治疗的患者 | 双能CT | 治疗的重度主动脉瓣狭窄患者在2.6年的中位随访期间,有15例全因死亡和11例因心力衰竭住院。在Kaplan-Meier分析中,高ECV组(≥27.8%)的复合结局发生率显著高于低ECV组(<27.8%)。在多变量回归分析中,ECV是不良结局的唯一独立预测因素。 | 86 |
| Hayashi et al | 2022 | 肺动脉高压 | 20例患者 | 双能量CT | ECV与前RVIP的平均PAP高度相关(r = 0.64),与后RVIP和间隔中度相关(r = 0.50-0.42)。 | 87 |
| Tu et al | 2022 | 化疗患者 | 1151例蒽环类药物化疗后出现心脏毒性患者 | 常规CT | 在基线、治疗期间和治疗后测量单能量胸部CT-ECV;在癌症治疗相关心功能不全中,6个月和12个月时的CT-ECV显著较高。 | 88 |
| Yashima et al | 2022 | 扩张型心肌病 | 70例患者 | 常规CT | ECV、收缩末期容积和重大瓣膜病发生率在MACE病例中显著较高(平均值分别为37.16% ± 5.91和2.59% ± 3.95;平均值分别为194 mL ± 109和138 mL ± 78;以及57%和20%;所有P <0.05)。仅CT-ECV是MACE的独立预测因素(P = 0.0468)。 | 89 |
| Kidoh et al | 2023 | 房颤 | 105例患者 | 未提供 | 持续性房颤患者的CT-ECV显著高于阵发性房颤患者(平均值,30% ± 5% vs 26% ± 5%; P < .001)。 | 59 |
上面的表的缩写如下:
-
AUC =受试者工作特征曲线下面积,area under the receiver operating characteristic curve -
BNP =脑利钠肽,brain natriuretic peptide -
NT-proBNP = 前激素状态脑利钠肽的N末端片段,N-terminal fragment of the prohormone BNP -
CAD =冠心病,coronary artery disease -
CPEPH =慢性肺栓塞相关肺动脉高压,chronic pulmonary embolism–related pulmonary hypertension -
PAP =肺动脉压, pulmonary artery pressure -
PVR =肺血管阻力,pulmonary vascular resistance -
LAV =左心房容积,left atrial volume -
LV =左心室,left ventricle -
LVEF =左心室射血分数,LV ejection fraction -
MACE =主要不良心脏事件,major adverse cardiac events -
RVIP =右心室插入点,right ventricular insertion point -
TAVR =经导管主动脉瓣置换术,transcatheter aortic valve replacement
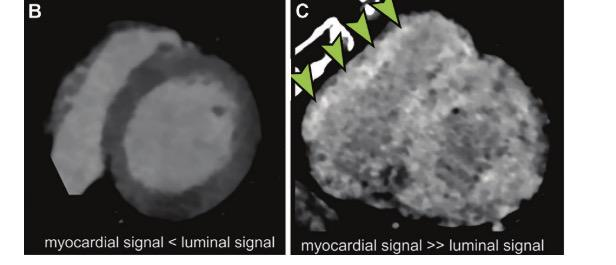
2024年发表在JCCT上的meta分析研究展示的CT-ECV如下(Ref 75):
-
健康受试者(Healthy):27.6%(95%CI 25.7%-29.4%) -
重度主动脉瓣狭窄(Aortic Stenosis):31.2%(95%CI 28.5-33.8%) -
非缺血性扩张型心肌病(Dilated Cardiomyopathy):36.9%(95%CI 31.6%-42.3%) -
心脏淀粉样变性(Cardiac Amyloidosis):50. 2%(95% CI 46. 2%-54. 2%)
不同人群的平均CT-ECV值比较见下图:
可以看到,
健康受试者和重度主动脉瓣狭窄受试者的平均CT-ECV值的95%置信区间存在重叠。
健康人
12项研究(248位患者)调研了无心血管疾病个体的研究及其特征:
| 作者 | 年 | 研究设计 | 平均ECV(%) | 健康患者数 | 平均年龄 | 男性(%) | 高血压(%) | BMI(kg/m2) | 糖尿病(%) | 血脂异常(%) | 吸烟史(%) | 延迟时间(min) | 算法供应商 | 范围 | Ref |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nacif | 2012 | 前瞻性常规CT扫描 | 21.6 | 11 | 58.8 ±5.3 | 63.6 | 36.3 | NA | 0 | 45.4 | 63.6 | 10 | Vitrea | 前心(Anterior) | 45 |
| Nacif | 2013 | 前瞻常规CT扫描 | 24.2 | 9 | 59 ± 7 | 44 | 22 | 27 | 0 | 44 | 89 | 7 | Vitrea | 全心 | 62 |
| Kurita | 2016 | 前瞻性常规CT扫描 | 25.4 | 38 | 65 ± 10 | 63 | 66 | 24.9 | 39 | 47 | 47 | 7 | Vitrea | 全心 | 64 |
| Lee | 2016 | 前瞻双能CT扫描 | 26.1 | 55 | 5.7 ± 8.8 | 57.1 | NA | NA | NA | NA | NA | 7 | Siemens | 全心 | 50 |
| Ohta | 2017 | 前瞻双能CT扫描 | 26.3 | 20 | 67.6 ± 8.8 | 60 | 8 | 21.7 | 15 | 40 | NA | 12 | GE | 隔膜 | 53 |
| Hamdy | 2019 | 回顾性常规CT扫描 | 26.8 | 17 | 67.5 ± 10 | 89 | 0 | NA | 0 | 0 | 0 | 7 | Ziosoft | 全心 | 47 |
| van Assen | 2019 | 回顾性双能CT扫描 | 27.1 | 9 | 66 ± 6 | 63 | 75 | 31.1 | 50 | 63 | 50 | 7 | Siemens | 全心 | 61 |
| Scully | 2020 | 回顾常规CT扫描 | 28.0 | 20 | 60 ± 11 | NA | NA | NA | NA | NA | NA | 5 | Siemens | 全心 | 48 |
| Abadia | 2020 | 回顾性双能CT扫描 | 29.2 | 10 | 60.6 ± 9.2 | 70 | NA | 29.6 | NA | NA | NA | 7 | Siemens | 全心 | 51 |
| Hammer | 2021 | 前瞻性常规CT扫描 | 29.3 | 19 | 57.2 ±5.6 | 36.8 | 26.3 | 27.6 | 15.8 | 52 | 31.6 | 5 | - | 隔膜 | 60 |
| Yamasaki | 2021 | 回顾性双能CT扫描 | 33.0 | 8 | 68 ± 7 | 50 | NA | NA | NA | NA | NA | 7 | Philips | 全心 | 63 |
| Qi | 2022 | 前瞻双能CT扫描 | 35.1 | 80 | 60.5 ±10.9 | 57.3 | 42.5 | 25.1 | 13.9 | 44.7 | 12.5 | 7 | Siemens | 全心 | 55 |
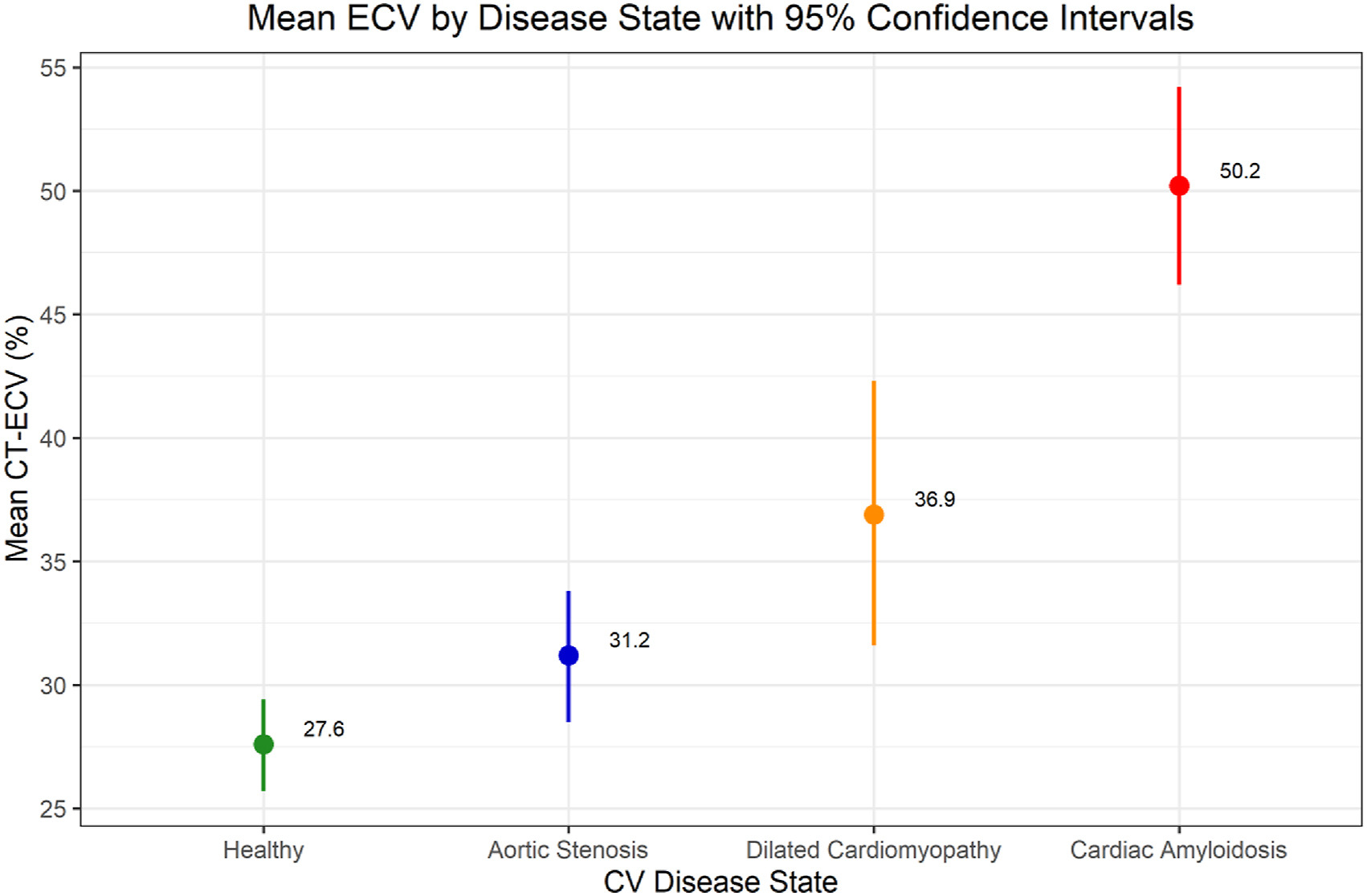
如下图所示,各研究中无疾病受试者的平均CT-ECV值的汇总估计值为27.6%(95%CI 25.7%-29.4%)

在正常人中,不同研究中的CT-ECV的差异可能来源有:
-
不同厂家的软件包 -
平衡期图像采集的时间延迟 -
CT的扫描模式(双能量/单能量) -
心肌感兴趣区域(使用心脏的局部进行计算/全心) -
造影剂差异 -
辐射剂量(管电流,管电压) -
图像重建方法 -
心脏CT采集的期相
主动脉狭窄
多项研究表明,ECV-CT显示对接受经导管主动脉瓣置换术(TAVR)或外科瓣膜置换术的患者结局具有预测价值。
以下9项研究共纳入804例受试者,评价了严重主动脉瓣狭窄患者的CT-ECV值:
| 作者 | 年 | 患者 | 研究人群描述 | 平均年龄 | 男性(%) | 平均ECV(%) | 95%置信区间 | Ref |
|---|---|---|---|---|---|---|---|---|
| Treibel | 2015 | 27 | 重度主动脉狭窄 | 68±8 | 70 | 28 | 26.5-29.5 | 72 |
| Scully | 2020 | 93 | TAVR前重度主动脉狭窄 | 85 ± 5 | 41 | 33 | 32.2-33.9 | 48 |
| Tamarappoo | 2020 | 150 | 低流量低梯度(LFLG)主动脉瓣狭窄患者 | 81±10 | 60 | 31.1 | 29.7-32.5 | 49 |
| Dubourg | 2021 | 21 | 主动脉置换术(AVR)前重度主动脉狭窄 | 86±4.9 | 50 | 29.9 | 20.9-48.3 | 54 |
| Hammer | 2021 | 75 | 主动脉置换术(AVR)前重度主动脉狭窄 | 80.6±6.8 | 47 | 40 | 37.5-42.5 | 60 |
| Han | 2021 | 109 | LVEF(左心室射血分数) <50%的重度主动脉狭窄TAVR术前 | 80±9.7 | 76 | 31.9 | 30.5-33.3 | 66 |
| Suzuki | 2021 | 95 | TAVR前重度主动脉狭窄 | 84 ± 5 | 25 | 28.1 | 27.3-28.9 | 67 |
| Koike | 2023 | 142 | TAVR前重度主动脉狭窄 | 81 ± 7.4 | 53 | 29.5 | 29.0-30.1 | 73 |
| Vignale | 2023 | 113 | TAVR前重度主动脉狭窄 | 82±4.5 | 48 | 28.4 | 27.6-29.2 | 74 |
纳入的研究的患者平均年龄范围为68-85岁。
严重主动脉瓣狭窄参与者的平均CT-ECV为31.2%(95%CI 28.5-33.8%),具有显著异质性(I2 = 96%)

Dubourg等人(Ref 54)探究了21 名重度主动脉瓣狭窄患者的双能CT-ECV和MR-ECV的关系:
-
与MR-ECV(29.1±3.9%)相比,CT-ECV(29.9±4.6 %) 略微高估了ECV(P<0.0001) -
按节段和按患者分析的偏差和一致性极限分别为+2.3%和+2.5%。
最新的研究表明,在重度主动脉瓣狭窄患者的经导管或外科瓣膜置换术后,CT-ECV与
-
NYHA分级 -
B型钠尿肽 -
超声心动图左心室射血分数E/e'比
显著相关,即较高的CT-ECV患者卒中和心力衰竭风险有所增加(Ref 74)。
Scully等人(Ref 48)在112例孤立性主动脉瓣狭窄(淀粉样变性除外)TAVR患者中发现,ECV增加2%,中期(> 1.5年)死亡风险加倍。
Han在109例主动脉瓣狭窄患者的研究表明,接受TAVR的重度主动脉瓣狭窄患者中,左心室射血分数恢复的患者的CT-ECV(29.4%)显著低于未恢复的患者(33.2%)(Ref 85)。
Suzuki在95例接受TAVR治疗的患者上的研究证明了,高ECV组(≥27.8%)的复合不良结局发生率显著高于低ECV组(<27.8%),ECV是不良结局的唯一独立预测因素(Ref 86)
在低流量低梯度主动脉瓣狭窄患者中,从术前TAVR计划CT扫描中获得的ECV增加(CT-ECV > 33%)是TAVR后心力衰竭和2年死亡率的重要预测因素(Ref 49)。
随访时,CT-ECV > 32%与左心室质量更缓慢的改善相关,CT-ECV是心力衰竭住院的最佳独立预测因子(Ref 70)。
Ishiyama等人在71例接受TAVR的重度主动脉瓣狭窄患者中证明,对接受 TAVR 的患者进行 CT-ECV 定量对预测左室射血分数(LVEF)的改善以及全因死亡和心衰住院率有预后益处(Ref 78)。
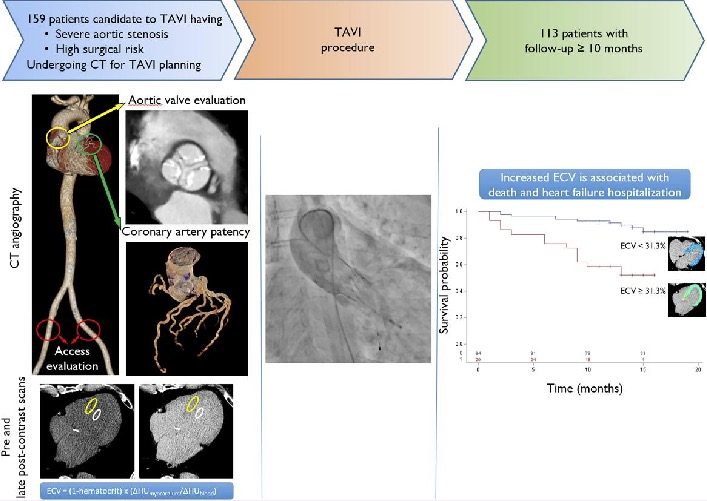
在113位重度主动脉瓣狭窄患者的前瞻性观察队列研究中,ECV高于31.3%与 随访时死亡或因心衰住院(heart failure hospitalization,HFH) 风险增加强相关,因此TAVI计划前的CT-ECV可预测HFH或死亡的复合终点(Ref 74)。
扩张型心肌病
4项研究(89例受试者)调查了非缺血性扩张型心肌病受试者的CT-ECV值。
| 作者 | 年 | 患者数 | 研究人群描述 | 平均年龄 | 男性(%) | 平均ECV(%) | 95%置信区间 | Ref |
|---|---|---|---|---|---|---|---|---|
| Lee | 2016 | 9 | 基于非缺血性扩张性心肌病 | NA | NA | 31.3 | 29.7-32.9 | 50 |
| Esposito | 2018 | 9 | 扩张型心肌病伴复发性室性心动过速 | 67±6 | 89 | 44 | 41.4-46.6 | 76 |
| Abadia | 2020 | 20 | 非缺血性扩张型心肌病 | 63.9±10.3 | 75 | 38.3 | 35.3-41.3 | 51 |
| Kim | 2022 | 51 | 非缺血性扩张型心肌病缺血性心肌病 | 59.9±15.6 | 51 | 34.5 | 32.6-36.4 | 77 |
各研究中扩张型心肌病的病例定义各不相同,
扩张型心肌病的平均CT-ECV值为36.9%(95%CI 31.6%-42.3%),具有显著的研究间异质性(I2 = 95.8%)

MACE,主要心血管事件,定义为死亡、室性心动过速或室颤和心力衰竭。
CT-ECV是扩张型心肌病患者随访时MACE的预测因子,以33%的CT-ECV作为临界值,以区分MACE的高风险和低风险患者 (Ref 77)
Abadia等人(Ref 51)的研究证明:
-
健康心肌、非缺血性心肌病和缺血性心肌病的CT-ECV 分别为 25.4%(22.9-27.3)、38.3%(33.7-43.0)和 36.9%(32.4-41.1)。 -
健康心肌的 ECV 值明显低于缺血和非缺血心肌病(P < 0.001)。
Esposito等人的研究纳入了复发性室性心动过速患者,其平均CT-ECV(44%) 较高,这可能与更晚期的疾病基质相关(Ref 76)。
心脏淀粉样变性
心脏淀粉样变(Cardiac Amyloidosis, CA)是由淀粉样蛋白(细胞外错误折叠的蛋白质)沉积于心肌间质的临床综合征。
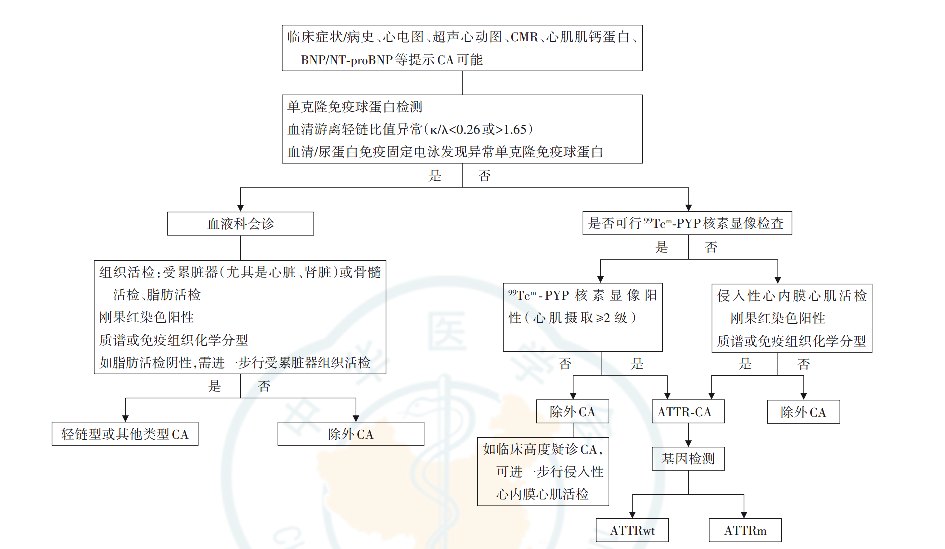
心脏淀粉样变性(Cardiac Amyloidosis, CA)的分类,详见中山一大内的这篇推文
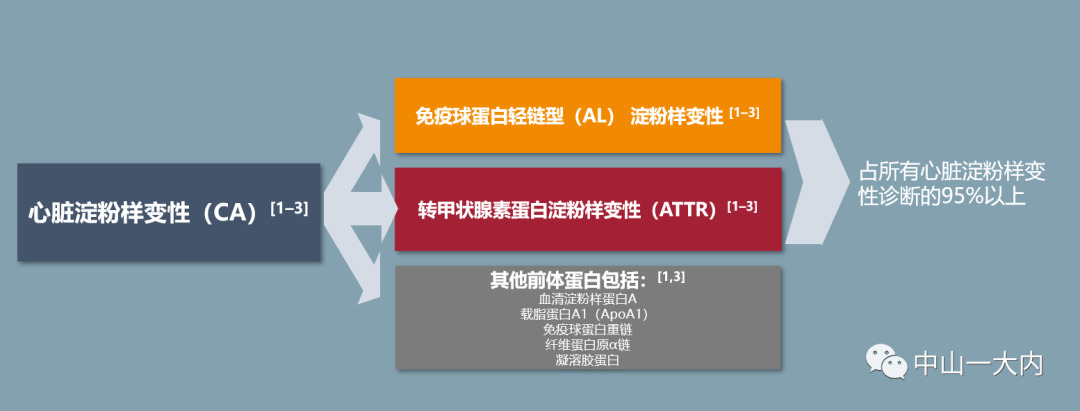
免疫球蛋白轻链(AL amyloidosis,Immunoglobulin light-chain amyloidosis,AL)、转甲状腺素蛋白 (transthyretin amyloid,TTR)、血清淀粉样蛋白A、血清载脂蛋白A1等均可导致CA。
其中最多见的是AL和TTR,占98%以上。
-
AL = AL amyloidosis,Immunoglobulin light-chain amyloidosis,免疫球蛋白轻链型淀粉样变性
关于免疫球蛋白轻链型淀粉样变性的内容,详见
-
ATTR = transthyretin amyloid,转甲状腺素蛋白淀粉样变性
关于转甲状腺素蛋白淀粉样变性的治疗共识,详见这个系列报道 目前,心脏淀粉样变性的检测主要依赖于心脏MR检测,
与心脏磁共振成像相比,
CT-ECV 可提供更快速、更便宜、更广泛的检查,
对于有磁共振成像禁忌症(如金属装置或肾脏疾病)的患者可能更有优势。
大规模的队列研究证实,CT-ECV 对心脏淀粉样变性(Cardiac Amyloidosis, CA)的检测和量化具有很高的诊断准确性。
以下汇总的5项研究共纳入159名参与者,检查了心脏淀粉样变性患者的CT-ECV值
(n =49例轻链淀粉样变性AL 和n=110例甲状腺素运载蛋白淀粉样变性 ATTR)。
| 作者 | 年 | 患者 | 研究人群描述 | 平均年龄 | 男性(%) | 平均ECV(%) | 95%置信区间 | Ref |
|---|---|---|---|---|---|---|---|---|
| Gama | 2022 | 72 | 35患有AL淀粉样蛋白,37患有ATTR淀粉样蛋白 | 67±5.2 | 71 | 49 | 45.8-52.2 | 71 |
| Kidoh | 2023 | 41 | 3患有AL淀粉样蛋白,38患有ATTR淀粉样蛋白 | 78±9 | 73 | 52 | 48.3-55.7 | 59 |
| Lee | 2016 | 4 | 3患有AL淀粉样蛋白,1例ATTR淀粉样蛋白 | NA | NA | 53.5 | 41.1-55.8 | 50 |
| Scully | 2020 | 16 | 16例ATTR淀粉样蛋白和重度AS | 88±5 | 56 | 43 | 40.1-46.0 | 48 |
| Treibel | 2015 | 26 | 8例AL淀粉样蛋白,18例ATTR淀粉样蛋白 | 64±14 | 81 | 54 | 49.8-58.2 | 72 |
备注:
-
AL = AL amyloidosis,Immunoglobulin light-chain amyloidosis,免疫球蛋白轻链型淀粉样变性 -
ATTR = transthyretin amyloid,转甲状腺素蛋白淀粉样变性
使用CT-ECV探究其在心脏淀粉样变性的研究的平均年龄范围为64 - 88岁。
心脏淀粉样变性(Cardiac Amyloidosis,CA)患者的总体CT-ECV值为50. 2%(95% CI 46. 2%-54. 2%),具有显著异质性(I2 = 88. 5%):
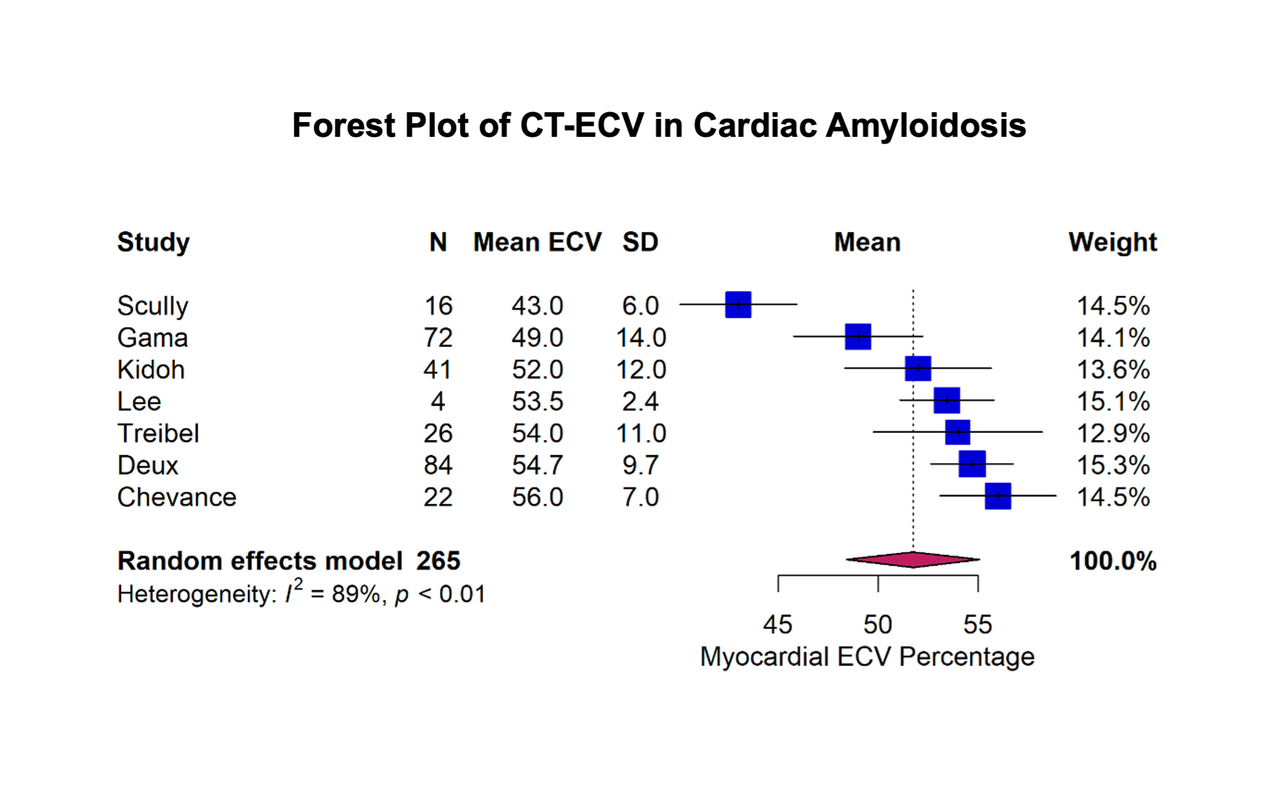
在几乎所有研究中,心脏淀粉样变性患者的CT-ECV都远远高于健康患者。
Deux等人的研究(Ref 57)表明:
-
心脏淀粉样变性的CT-ECV(54.7% ± 9.7%)高于非淀粉样蛋白性心脏肥大患者(34.6% ± 9.1%;P < .001)和无肥厚患者(35.9% ± 9.9%;P = .001)。 -
在确诊为系统性淀粉样变性和可变心脏受累的患者中,CT-ECV与不良心脏重塑相关。 -
CT-ECV与甲状腺素运载蛋白(而非轻链)淀粉样蛋白(ATTR)患者的全因死亡率独立相关。
急诊
近年来,由于能够快速排除冠状动脉主动脉和肺动脉同时成像的疾病,
CCTA在急诊中的作用越来越大。
然而,
存在冠状动脉通畅的急性心脏病,例如急性心肌炎、冠状动脉未阻塞的心肌梗死和各种心肌病,不能单独通过(动脉期)CCTA完成诊断。
CT-ECV的另一个潜在的应用是识别和表征急性胸痛和心肌肌钙蛋白升高患者的心肌损伤。
在这种临床情况下,
实施平衡期碘增强的瘢痕检测和CT-ECV评估,可能有利于更早地建立正确的诊断,缩短住院时间,避免不必要的下游检查,从而降低医疗保健系统的总体成本(Ref 76)。
因此,Palmisano等人最近提出了一种胸痛方案,若在CCTA中无法准确地对疾病进行定位时,额外在造影剂注射后10min进行平衡期的扫描(Ref 79)。
在上述研究中评估了84例急性胸痛患者,其中42例CCTA无发现的患者进行了平衡期扫描。
使用动脉期和平衡期的CCTA可以对上述患者进行诊断,分别为:
-
心肌炎(52%) -
Takotsubo心肌病(10%) -
淀粉样变性(7%) -
冠状动脉未阻塞的心肌梗死(7%) -
扩张型心肌病(5%)
Si-Mohamed等人(Ref 65)在最新的双能光子CT上探究了CT-ECV在诊断急性心肌炎方面的应用价值,
研究表明心肌炎患者的CT-ECV为31.60% ,显著高于对照组(健康人)CT-ECV,AUC为0.835 。
更多阅读
以上就是CT-ECV科研相关的全部内容了。
在下期将会为大家带来心肌应力分析,Cardiac CT Myocardial Strain的相关内容。
#141 冠状动脉粥样硬化
-
指南文件 -
大规模临床试验 -
AI斑块分析软件 -
CAD-RADS 2.0
#142 非入侵的心脏病理
-
指南文件 -
FFR -
心肌CT灌注
#143 结构性心脏病
-
结构性心脏病 -
CT应用于TAVI -
CT应用于二尖瓣和三尖瓣的治疗 -
CT应用于瓣膜植入术后
#147 细胞外容积分数基础
-
ECV的计算原理——平衡期、计算、ROI勾画 -
ECV的扫描协议——延长时间、造影剂、辐射剂量
参考文献
-
Dodd JD, Leipsic JA. Evolving Developments in Cardiac CT. Radiology. 2023;307(3):e222827. doi:10.1148/radiol.222827 -
Writing Committee Members; Gulati M, Levy PD, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/ SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021;78(22):2218–2261. -
Adamson PD, Williams MC, Dweck MR, et al. Guid- ing Therapy by Coronary CT Angiography Improves Outcomes in Patients With Stable Chest Pain. J Am Coll Cardiol 2019;74(16):2058–2070. -
DISCHARGE Trial Group; Maurovich-Horvat P, Bosserdt M, et al. CT or Invasive Coronary Angiography in Stable Chest Pain. N Engl J Med 2022;386(17):1591–1602. -
Lee SE, Sung JM, Andreini D, et al. Differential association between the pro- gression of coronary artery calcium score and coronary plaque volume pro- gression according to statins: the Progression of AtheRosclerotic PlAque DetermIned by Computed TomoGraphic Angiography Imaging (PARADIGM) study. Eur Heart J Cardiovasc Imaging 2019;20(11):1307–1314. -
Han D, Chen B, Gransar H, et al. Prognostic significance of plaque location in non-obstructive coronary artery disease: from the CONFIRM registry. Eur Heart J Cardiovasc Imaging 2022;23(9):1240–1247. -
Patel AR, Bamberg F, Branch K, et al. Society of cardiovascular computed tomography expert consensus document on myocardial computed tomography perfusion imaging. J Cardiovasc Comput Tomogr 2020;14(1):87–100. -
Blanke P, Weir-McCall JR, Achenbach S, et al. Computed tomography imag- ing in the context of transcatheter aortic valve implantation (TAVI) / transcatheter aortic valve replacement (TAVR): An expert consensus document of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr 2019;13(1):1–20. -
Boogers MJ, Broersen A, van Velzen JE, de Graaf FR, El-Naggar HM, Kitslaar PH, et al. Automated quantification of coronary plaque with computed tomography: comparison with intravascular ultrasound using a dedicated registration algorithm for fusion-based quantification. Eur Heart J 2012;33:1007-1016 -
de Graaf MA, Broersen A, Kitslaar PH, Roos CJ, Dijkstra J, Lelieveldt BP, et al. Automatic quantification and characterization of coronary atherosclerosis with computed tomography coronary angiography: cross-correlation with intravascular ultrasound virtual histology. Int J Cardiovasc Imaging 2013;29:1177-1190 -
Fujimoto S, Kondo T, Kodama T, Fujisawa Y, Groarke J, Kumamaru KK, et al. A novel method for non-invasive plaque morphology analysis by coronary computed tomography angiography. Int J Cardiovasc Imaging 2014;30:1373-1382 -
Voros S, Rinehart S, Qian Z, Vazquez G, Anderson H, Murrieta L, et al. Prospective validation of standardized, 3-dimensional, quantitative coronary computed tomographic plaque measurements using radiofrequency backscatter intravascular ultrasound as reference standard in intermediate coronary arterial lesions: results from the ATLANTA (assessment of tissue characteristics, lesion morphology, and hemodynamics by angiography with fractional flow reserve, intravascular ultrasound and virtual histology, and noninvasive computed tomography in atherosclerotic plaques) I study. JACC Cardiovasc Interv 2011;4:198-208 -
Choi AD, Marques H, Kumar V, Griffin WF, Rahban H, Karlsberg RP, et al. CT evaluation by artificial intelligence for atherosclerosis, stenosis and vascular morphology (CLARIFY): a multi-center, international study. J Cardiovasc Comput Tomogr 2021;15:470-476 -
Sheahan M, Ma X, Paik D, Obuchowski NA, St Pierre S, Newman WP 3rd, et al. Atherosclerotic plaque tissue: noninvasive quantitative assessment of characteristics with software-aided measurements from conventional CT angiography. Radiology 2018;286:622-631 -
Dey D, Schepis T, Marwan M, Slomka PJ, Berman DS, Achenbach S. Automated three-dimensional quantification of noncalcified coronary plaque from coronary CT angiography: comparison with intravascular US. Radiology 2010;257:516-522 -
Tzimas G, Gulsin GS, Everett RJ, Akodad M, Meier D, Sewnarain K, et al. Age- and sex-specific nomographic CT quantitative plaque data from a large international cohort. JACC Cardiovasc Imaging 2024;17:165-175 -
Tzimas G. Nomographic CT quantitative plaque data from a large international population. Society of Cardiovascular Computed Tomography Annual Meeting, Las Vegas, 2022. https://cdn.ymaws.com/scct.org/resource/resmgr/ scct_2022_printed_program_AB.pdf. -
Cury RC, Leipsic J, Abbara S, et al. CAD-RADSTM 2.0 - 2022 Coronary Artery Disease-Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR), and the North America Society of Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr 2022;16(6):536–557. -
Curzen N, Nicholas Z, Stuart B, et al. Fractional flow reserve derived from computed tomography coronary angiography in the assessment and management of stable chest pain: the FORECAST randomized trial. Eur Heart J. 2021;42(37):3844-3852. doi:10.1093/eurheartj/ehab444IF: 37.6 Q1 -
Nanna MG, Vemulapalli S, Fordyce CB, et al. The prospective randomized trial of the optimal evaluation of cardiac symptoms and revascularization: Rationale and design of the PRECISE trial. Am Heart J. 2022;245:136-148. doi:10.1016/j.ahj.2021.12.004IF: 3.7 Q1 -
Bech GJW, De Bruyne B, Pijls NH, et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation 2001; 103:2928–2934 -
Tonino PAL, De Bruyne B, Pijls NHJ, et al.; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009; 360:213–224 -
De Bruyne B, Pijls NHJ, Kalesan B, et al.; FAME 2 Trial Investigators. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med 2012; 367:991–1001 -
Takx RA, Blomberg BA, El Aidi H, Habets J, et al. Diagnostic accuracy of stress myocardial perfusion imaging compared to invasive coronary angiography with fractional flow reserve met- analysis. Circ Cardiovasc Imaging 2015;8:1–7. -
Koo BK, Erglis A, Doh JH, et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multi-center DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J Am Coll Cardiol 2011; 58:1989–1997 -
Min JK, Leipsic J, Pencina MJ, et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA 2012; 308:1237–1245 -
Nørgaard BL, Leipsic J, Gaur S, et al.; NXT Trial Study Group. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (analysis of coronary blood flow using CT angiography: next steps). J Am Coll Cardiol 2014; 63:1145–1155 -
Griffin WF, Choi AD, Riess JS, et al. AI Evaluation of Stenosis on Coronary CTA, Comparison With Quantitative Coronary Angiography and Fractional Flow Reserve: A CREDENCE Trial Substudy. JACC Cardiovasc Imaging. 2023;16(2):193–205. doi: 10.1016/j.jcmg.2021.10.020. -
Madsen KT, Nørgaard BL, Øvrehus KA, et al. Prognostic Value of Coronary CT Angiography-derived Fractional Flow Reserve on 3-year Outcomes in Patients with Stable Angina. Radiology. 2023;308(3):e230524. doi: 10.1148/radiol.230524. -
Cherukuri L, Birudaraju D, Kinninger A, et al. Use of Advanced CT Technology to Evaluate Left Atrial Indices in Patients with a High Heart Rate or with Heart Rate Variability: The Converge Registry. J Nucl Med Technol. 2021;49(1):65–69. doi: 10.2967/jnmt.120.253781. -
Sand NPR, Veien KT, Nielsen SS, et al. Prospective comparison of FFR de- rived from coronary CT angiography with SPECT perfusion imaging in stable coronary artery disease: the ReASSESS study. JACC Cardiovasc Imaging 2018; 11:1640–1650 -
Artzner C, Daubert M, Ehieli W, et al. Impact of computed tomography (CT)-derived fractional flow reserve on reader confidence for interpreta- tion of coronary CT angiography. Eur J Radiol 2018; 108:242–248 -
Curzen NP, Nolan J, Zaman AG, Nørgaard BL, Rajani R. Does the routine availability of CT-derived FFR influence management of patients with stable chest pain compared to CT angiography alone? The CT-FFR RIPCORD study. JACC Cardiovasc Imaging 2016; 9:1188–1194 -
Douglas PS, Pontone G, Hlatky MA, et al.; PLATFORM Investigators. Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT)— outcome and resource impacts study. Eur Heart J 2015; 36:3359–3367 -
Andreini D, Modolo R, Katagiri Y, et al.; SYNTAX III REVOLUTION Investiga- tors. Impact of fractional flow reserve derived from coronary computed tomography angiography on heart team treatment decision-making in patients with multivessel coronary artery disease: insights from the SYNTAX III REVOLUTION trial. Circ Cardiovasc Interv 2019; 12:e007607 -
Dewey M, Siebes M, Kachelrieß M, et al. Clinical quantitative cardiac imaging for the assessment of myocardial ischaemia. Nat Rev Cardiol 2020;17(7):427–450. -
Nous FMA, Geisler T, Kruk MBP, et al. Dynamic Myocardial Perfusion CT for the Detection of Hemodynamically Significant Coronary Artery Disease. JACC Cardiovasc Imaging 2022;15(1):75–87. -
Andreini D, Mushtaq S, Pontone G, et al. CT Perfusion Versus Coronary CT Angiography in Patients With Suspected In-Stent Restenosis or CAD Progres- sion. JACC Cardiovasc Imaging 2020;13(3):732–742. -
Narula J, Chandrashekhar Y, Ahmadi A, et al. SCCT 2021 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr 2021;15(3):192–217. -
中华医学会放射学分会心胸学组, 国家心血管病专业质控中心心血管影像质控专家工作组 . 动态 CT 心肌灌注成像技术操作与图像分析中国专家共识[J]. 中华放射学杂志, 2022, 56(12): 1289-1299. DOI: 10.3760/cma.j.cn112149-20220308-00213. -
Rudzinski PN, Leipsic JA, Schoepf UJ, et al. CT in Transcatheter-delivered Treatment of Valvular Heart Disease. Radiology. 2022;304(1):4-17. doi:10.1148/radiol.210567 -
Fam NP, von Bardeleben RS, Hensey M, et al. Transfemoral Transcatheter Tricuspid Valve Replacement With the EVOQUE System: A Multicenter, Observational, First-in-Human Experience. JACC Cardiovasc Interv 2021;14(5):501–511. -
Reid A , Ben ZekryS , Turaga M, et al . Neo-LVOT and Transcatheter Mitral Valve Replacement: Expert Recommendations. JACC Cardiovasc Imaging 2021;14(4):854–866. -
Hensey M, Alenezi AR, Murdoch DJ, et al. Transcatheter Tricuspid Valve-in- Valve Replacement With Subsequent Bioprosthetic Valve Fracture to Opti- mize Hemodynamic Function. JACC Cardiovasc Interv 2018;11(21):2226– 2227. -
Nacif MS, Kawel N, Lee JJ et al (2012) Interstitial myocardial fibrosis assessed as extracellular volume fraction with low-radiation-dose cardiac CT. Radiology 264:876–883. -
Bandula S, White SK, Flett AS et al (2013) Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: validation against histologic findings. Radiology 269:396–403. -
Hamdy A, Kitagawa K, Goto Y et al (2019) Comparison of the different imaging time points in delayed phase cardiac CT for myocardial scar assessment and extracellular volume fraction estimation in patients with old myocardial infarction. Int J Cardiovasc Imaging 35:917–926. -
Scully PR, Patel KP, Saberwal B et al (2020) Identifying cardiac amyloid in aortic stenosis. JACC Cardiovasc Imaging 13:2177–2189. -
Tamarappoo B, Han D, Tyler J et al (2020) Prognostic value of computed tomography–derived extracellular volume in tavr patients with low-flow low-gradient aortic stenosis. JACC Cardiovasc Imaging 13:2591–2601. -
Lee H-J, Im DJ, Youn J-C et al (2016) Myocardial extracellular volume fraction with dual-energy equilibrium contrast-enhanced cardiac CT in nonischemic cardiomyopathy: a prospective comparison with cardiac MR imaging. Radiology 280:49–57. -
Abadia AF, van Assen M, Martin SS et al (2020) Myocardial extracellular volume fraction to differentiate healthy from cardiomyopathic myocardium using dual-source dual-energy CT. J Cardiovasc Comput Tomogr 14:162–167. -
Oda S, Emoto T, Nakaura T et al (2019) Myocardial late iodine enhancement and extracellular volume quantification with dual-layer spectral detector dual-energy cardiac CT. Radiol Cardiothorac Imaging 1:e180003. -
Ohta Y, Kishimoto J, Kitao S et al (2020) Investigation of myocardial extracellular volume fraction in heart failure patients using iodine map with rapid-kV switching dual-energy CT: segmental comparison with MRI T1 mapping. J Cardiovasc Comput Tomogr 14:349–355. -
Dubourg B, Dacher J-N, Durand E et al (2021) Single-source dual energy CT to assess myocardial extracellular volume fraction in aortic stenosis before transcatheter aortic valve implantation (TAVI). Diagn Interv Imaging 102:561–570. -
Qi R-X, Jiang J-S, Shao J et al (2022) Measurement of myocardial extracellular volume fraction in patients with heart failure with preserved ejection fraction using dual-energy computed tomography. Eur Radiol 32:4253–4263. -
Mergen V, Sartoretti T, Klotz E et al (2022) Extracellular volume quantification with cardiac late enhancement scanning using dual-source photon-counting detector CT. Invest Radiol 57:406–411. -
Deux JF, Nouri R, Tacher V, et al. Diagnostic Value of Extracellular Volume Quantification and Myocardial Perfusion Analysis at CT in Cardiac Amyloidosis. Radiology. 2021;300(2):326-335. -
Palmisano A, Vignale D, Tadic M, et al. Myocardial Late Contrast Enhancement CT in Troponin-Positive Acute Chest Pain Syndrome. Radiology. 2022;302(3):545-553. -
Kidoh, M., et al., Cardiac MRI-derived Extracellular Volume Fraction versus Myocardium-to-Lumen R1 Ratio at Postcontrast T1 Mapping for Detecting Cardiac Amyloidosis. Radiol Cardiothorac Imaging, 2023. 5(2): p. e220327. -
Hammer Y, Talmor-Barkan Y, Abelow A, et al. Myocardial extracellular volume quantification by computed tomography predicts outcomes in patients with severe aortic stenosis. PLoS One. 2021;16(3):e0248306. Published 2021 Mar 10. doi:10.1371/journal.pone.0248306 -
van Assen M, De Cecco CN, Sahbaee P, et al. Feasibility of extracellular volume quantification using dual-energy CT. J Cardiovasc Comput Tomogr. 2019;13(1):81-84. doi:10.1016/j.jcct.2018.10.011 -
Nacif M.S.,Liu Y.,Yao J. et al. 3D left ventricular extracellular volume fraction by low-radiation dose cardiac CT: assessment of interstitial myocardial fibrosis. Journal of Cardiovascular Computed Tomography. 2013 Jan 1; 7: 51-57 -
Yamasaki Y, Abe K, Kamitani T, et al. Right Ventricular Extracellular Volume with Dual-Layer Spectral Detector CT: Value in Chronic Thromboembolic Pulmonary Hypertension. Radiology. 2021;298(3):589-596. doi:10.1148/radiol.2020203719 -
Kurita Y, Kitagawa K, Kurobe Y, et al. Estimation of myocardial extracellular volume fraction with cardiac CT in subjects without clinical coronary artery disease: A feasibility study. J Cardiovasc Comput Tomogr. 2016;10(3):237-241. doi:10.1016/j.jcct.2016.02.001 -
Si-Mohamed SA, Restier LM, Branchu A, et al. Diagnostic Performance of Extracellular Volume Quantified by Dual-Layer Dual-Energy CT for Detection of Acute Myocarditis. J Clin Med 2021;10(15):3286. -
Han D, Tamarappoo B, Klein E, et al. Computed tomography angiographyderived extracellular volume fraction predicts early recovery of left ventricular systolic function after transcatheter aortic valve replacement. Eur Heart J Cardiovasc Imaging 2021;22(2):179–185. -
Suzuki M, Toba T, Izawa Y, et al. Prognostic Impact of Myocardial Extracellular Volume Fraction Assessment Using Dual-Energy Computed Tomography in Patients Treated With Aortic Valve Replacement for Severe Aortic Stenosis. J Am Heart Assoc 2021;10(18):e020655. -
Hayashi H, Oda S, Emoto T, et al. Myocardial extracellular volume quantification by cardiac CT in pulmonary hypertension: Comparison with cardiac MRI. Eur J Radiol 2022;153:110386. -
Tu C, Shen H, Liu R, et al. Myocardial extracellular volume derived from contrastenhanced chest computed tomography for longitudinal evaluation of cardiotoxicity in patients with breast cancer treated with anthracyclines. Insights Imaging 2022;13(1):85. -
Yashima S, Takaoka H, Iwahana T, et al. Evaluation of extracellular volume by computed tomography is useful for prediction of prognosis in dilated cardiomyopathy. Heart Vessels 2022;38(2):185–194. -
Gama F, Rosmini S, Bandula S, et al. Extracellular Volume Fraction by Computed Tomography Predicts Long-Term Prognosis Among Patients With Cardiac Amyloidosis. JACC Cardiovasc Imaging. 2022;15(12):2082-2094. doi:10.1016/j.jcmg.2022.08.006 -
Treibel TA, Bandula S, Fontana M, et al. Extracellular volume quantification by dynamic equilibrium cardiac computed tomography in cardiac amyloidosis. J Cardiovasc Comput Tomogr. 2015;9(6):585-592. doi:10.1016/j.jcct.2015.07.001IF: 5.5 Q1 -
Koike H, Cheng VY, Lesser A, et al. Importance of imaging-acquisition protocol and post-processing analysis for extracellular volume fraction assessment by computed tomography. J Cardiovasc Comput Tomogr. 2023;17(3):222-225. -
Vignale D, Palmisano A, Gnasso C, et al. Extracellular volume fraction (ECV) derived from pre-operative computed tomography predicts prognosis in patients undergoing transcatheter aortic valve implantation (TAVI). Eur Heart J Cardiovasc Imaging. 2023;24(7):887-896. doi:10.1093/ehjci/jead040 -
Muthalaly RG, Tan S, Nelson AJ, et al. Variation of computed tomography-derived extracellular volume fraction and the impact of protocol parameters: A systematic review and meta-analysis. J Cardiovasc Comput Tomogr. Published online June 14, 2024. doi:10.1016/j.jcct.2024.06.002 -
Esposito A, Palmisano A, Antunes S, et al. Assessment of Remote Myocardium Heterogeneity in Patients with Ventricular Tachycardia Using Texture Analysis of Late Iodine Enhancement (LIE) Cardiac Computed Tomography (cCT) Images. Mol Imaging Biol. 2018;20(5):816-825. doi:10.1007/s11307-018-1175-1 -
Kim NY, Im DJ, Youn JC, et al. Synthetic Extracellular Volume Fraction Derived Using Virtual Unenhanced Attenuation of Blood on Contrast-Enhanced Cardiac Dual-Energy CT in Nonischemic Cardiomyopathy. AJR Am J Roentgenol. 2022;218(3):454-461. doi:10.2214/AJR.21.26654 -
Ishiyama M, Kurita T, Takafuji M, et al. The cardiac computed tomography-derived extracellular volume fraction predicts patient outcomes and left ventricular mass reductions after transcatheter aortic valve implantation for aortic stenosis. J Cardiol. 2023;81(5):476-484. doi:10.1016/j.jjcc.2022.12.002 -
Palmisano A, Vignale D, Tadic M et al (2022) Myocardial late contrast enhancement CT in troponin-positive acute chest pain syndrome. Radiol-ogy 302:545–553. https:// doi. org/ 10. 1148/ radiol. 211288
本文由 mdnice 多平台发布


















 被折叠的 条评论
为什么被折叠?
被折叠的 条评论
为什么被折叠?
 到【灌水乐园】发言
到【灌水乐园】发言









