






Title
题目
Multidimensional Analysis of the Adult Human Heart in Health and Disease Using Hierarchical Phase-Contrast Tomography
使用分层相位对比断层扫描对成人健康和疾病状态下的心脏进行多维分析
Background
背景
Current clinical imaging modalities such as CT and MRI provide resolution adequate to diagnose cardiovascular diseases but cannot depict detailed structural features in the heart across length scales. Hierarchical phase-contrast tomography (HiP-CT) uses fourth-generation synchrotron sources with improved x-ray brilliance and high energies to provide micron-resolution imaging of intact adult organs with unprecedented detail.
目前的临床成像技术如CT和MRI能够提供足够的分辨率来诊断心血管疾病,但无法描绘心脏在不同长度尺度上的详细结构特征。分层相位对比断层扫描(HiP-CT)利用第四代同步辐射源,其X射线亮度和高能量得到了改善,能够以微米级分辨率成像完整的成人器官,提供前所未有的细节。
Method
方法
Between February 2021 and September 2023, two adult human donor hearts were obtained, fixed in formalin, and prepared using a mixture of crushed agar in a 70% ethanol solution. One heart was from a 63-year-old White male without known cardiac disease, and the other was from an 87-year-old White female with a history of multiple known cardiovascular pathologies including ischemic heart disease, hypertension, and atrial fibrillation. Nondestructive ex vivo imaging of these hearts without exogenous contrast agent was performed using HiP-CT at the European Synchrotron Radiation Facility.
在2021年2月至2023年9月期间,获得了两颗成人捐赠者的心脏,这些心脏在福尔马林中固定,并使用70%乙醇溶液中的碎琼脂混合物进行处理。其中一颗心脏来自一位63岁的白人男性,无已知心脏病;另一颗心脏来自一位87岁的白人女性,具有多种已知心血管病史,包括缺血性心脏病、高血压和心房颤动。使用欧洲同步辐射设施的HiP-CT对这些心脏进行了无损体外成像,未使用外源性对比剂
Conclusion
结论
HiP-CT provided high-spatial-resolution, three-dimensional images of structurally normal and diseased ex vivo adult human hearts. Whole-heart image volumes were obtained with isotropic voxels of approximately 20 µm, and local regions of interest were obtained with resolution down to 2.3–6.4 µm without the need for sectioning, destructive techniques, or exogenous contrast agents.
HiP-CT提供了结构正常和病变的体外成人心脏的高空间分辨率三维图像。整颗心脏的图像体积以各向同性体素约20微米的分辨率获得,而局部感兴趣区域的分辨率可达2.3至6.4微米,无需切片、破坏性技术或外源性对比剂。
Results
结果
HiP-CT demonstrated the capacity for high-spatial-resolution, multiscale cardiac imaging ex vivo, revealing histologic-level detail of the myocardium, valves, coronary arteries, and cardiac conduction system across length scales. Virtual sectioning of the cardiac conduction system provided information on fatty infiltration, vascular supply, and pathways between the cardiac nodes and adjacent structures. HiP-CT achieved resolutions ranging from gross (isotropic voxels of approximately 20 µm) to microscopic (approximately 6.4-µm voxel size) to cellular (approximately 2.3-µm voxel size) in scale. The potential for quantitative assessment of features in health and disease was demonstrated.
HiP-CT展示了高空间分辨率的多尺度心脏成像能力,能够在体外揭示心肌、瓣膜、冠状动脉和心脏传导系统的组织学级别细节。心脏传导系统的虚拟切片提供了有关脂肪浸润、血管供应以及心脏结节与邻近结构之间路径的信息。HiP-CT实现了从宏观(各向同性体素约20微米)到微观(体素大小约6.4微米)到细胞级别(体素大小约2.3微米)的分辨率。展示了在健康和疾病状态下对特征进行定量评估的潜力。
Figure
图
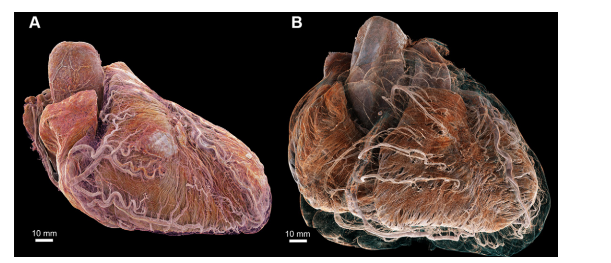
Figure 1: Three-dimensional cinematic renderings of the (A) control and (B) diseased hearts in anatomic orientation. Epicardial fat has been removed digitally to show the course of the major coronary arteries plus details of smaller arteries penetrating into the myocardium that are not typically seen on clinical CT scans. In the control heart, the coronary arteries remain close to the epicardial surface, while in the diseased heart, they are lifted away by epicardial fat, increasing the perfusion distance between the major coronary arteries and the myocardium. Segmentations and high-spatial-resolution details of coronary arteries in the diseased heart are also shown in Figure 5.
图1: 按解剖方向显示的(A)对照心脏和(B)病变心脏的三维电影渲染图。为了展示主要冠状动脉的路径及穿入心肌的较小动脉的细节,已数字化去除心外膜脂肪,这些细节在临床CT扫描中通常不可见。在对照心脏中,冠状动脉靠近心外膜表面,而在病变心脏中,冠状动脉被心外膜脂肪抬离,使主要冠状动脉和心肌之间的灌注距离增加。病变心脏的冠状动脉分割和高空间分辨率细节也在图5中展示。
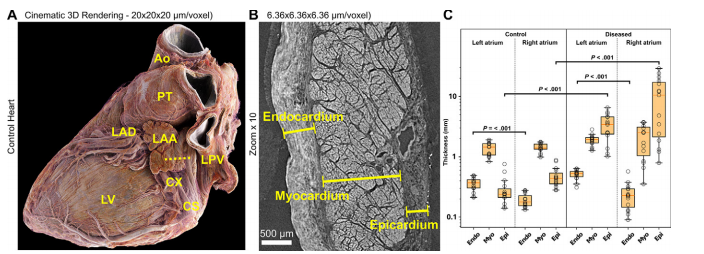
Figure 2: (A) Three-dimensional (3D) cinematic rendering from hierarchical phase-contrast tomography (HiP-CT) of the control heart, viewed from the left posterior aspect, with epicardial fat digitally removed using thresholding, shows the left atrium and the left atrial appendage (LAA), which can be seen running over the circumflex coronary artery (CX). This anatomic relationship is a key landmark for interventional closure of the left atrial appendage with devices. Ao = aorta, CS = coronary sinus, LAD = left anterior descending coronary artery, LPV = left pulmonary vein, LV = left ventricle, PT = pulmonary trunk. (B) High-spatial-resolution local HiP-CT scan of the wall of the left atrial appendage in the control heart (view plane is given by the dashed line in A) shows histologic spatial resolution of endocardial, myocardial, and epicardial layers, allowing measurement of thickness (lines). (C) Box and whiskers plots show the thickness of the endocardium (Endo), myocardium (Myo), and epicardium (Epi) in the left and right atria in the control heart and the diseased heart. Circles indicate individual measurements, the boundaries of boxes indicate the lower and upper quartiles, the red lines indicate medians, and the whiskers indicate ranges. Measurements were obtained manually at 15 distinct locations along the left and right atrial walls. Thickness measurements in the control and diseased hearts, and in right versus left atrium, were compared using unpaired multiple t tests with multiple comparison correction applied via the Holm-Sidak method and a set α threshold of .05. Statistical analysis revealed significant differences (P < .001) in the thickness of the left and right atrial endocardium within the control heart and within the diseased heart and in the thickness of the left and right atrial epicardium between the control heart and the diseased heart.
图2: (A) 从左后侧视角的对照心脏的三维(3D)电影渲染图,使用分层相位对比断层扫描(HiP-CT)技术,通过阈值处理数字化去除心外膜脂肪,显示左心房和左心耳(LAA),可见其运行在回旋冠状动脉(CX)上方。这个解剖关系是用设备进行左心耳介入闭合的关键标志。Ao = 主动脉,CS = 冠状窦,LAD = 左前降支冠状动脉,LPV = 左肺静脉,LV = 左心室,PT = 肺动脉干。(B) 对照心脏左心耳壁的高空间分辨率局部HiP-CT扫描(A中虚线所示的视平面)显示了心内膜、心肌层和心外膜层的组织学空间分辨率,允许测量厚度(线条)。(C) 盒须图显示了对照心脏和病变心脏左心房和右心房心内膜(Endo)、心肌层(Myo)和心外膜(Epi)的厚度。圆圈表示个别测量值,盒子的边界表示下四分位数和上四分位数,红线表示中位数,须表示范围。在左心房和右心房壁的15个不同位置手动获得的厚度测量值。使用未经配对的多重t检验比较对照心脏和病变心脏的厚度测量值,并通过Holm-Sidak方法应用多重比较校正,设定α阈值为.05。统计分析显示,对照心脏和病变心脏的左心房和右心房心内膜厚度,以及对照心脏和病变心脏左心房和右心房心外膜厚度之间存在显著差异(P < .001)。
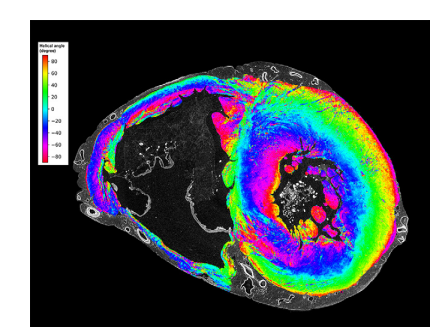
Figure 3: Mid-ventricular short-axis section of the ventricles in the control heart shows the feasibility of myomapping the orientation of myocyte aggregates on hierarchical phase-contrast tomography images at low spatial resolution. Myocyte orientation was calculated by means of structure tensor analysis with an in-house code based on the Python library structure-tensor (5,6). Colors represent the helical angle of aggregates of myocytes, which show a gradual transition in the thicker left ventricle from epicardium to endocardium.
图3: 对照心脏中室中段短轴切面显示了在低空间分辨率分层相位对比断层扫描图像上进行心肌细胞集群方向映射的可行性。心肌细胞方向是通过结构张量分析计算的,使用基于Python库structure-tensor的内部代码(5,6)。颜色代表心肌细胞集群的螺旋角度,显示在较厚的左心室中从心外膜到心内膜的逐渐过渡。
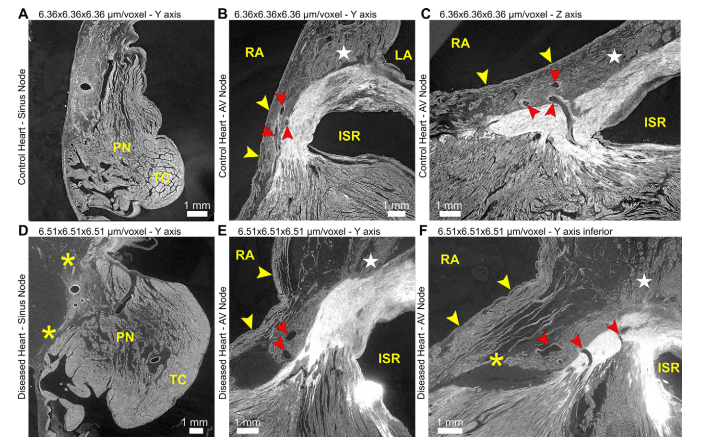
Figure 4: Hierarchical phase-contrast tomography images show the feasibility of identifying and tracing the conduction system with virtual multiplanar sectioning in (A–C)control and (D–F) diseased heart. In the control heart, the sinus and atrioventricular nodes are tightly adjacent to the surrounding atrial myocardium, paranodal area (PN), and terminal crest (TC), with multiple potential sites of connection. Multiplanar sectioning allows vascular connections from the atrioventricular node to be followed (red arrowheads in B, C, E, F). These connections can be seen breaking up the bright fibrous tissue between atrial and ventricular myocardium and represent potential sites of normal nodoventricular connection. In the diseased heart, there is fatty infiltration in the region of the sinus and atrioventricular nodes, separating the respective nodal tissue from surrounding right atrial (RA) myocardium (yellow arrowheads in B, C, E, F) and from the paranodal area. This fatty infiltration elongates the connections between nodal tissue and surrounding atrial myocardium ( in D). In particular, the connection between the atrioventricular node and the atrial septum (★ in B, C, E, F), a potential fast pathway, is diminished in the diseased heart compared with the control heart. An attenuated connection with the vestibule of the right atrium (potential slow pathway) can also be seen in a more inferior section of the diseased heart, made across the inferior pyramidal space ( in F). ISR = inferoseptal recess (within the left ventricle), LA = left atrium.
图4: 分层相位对比断层扫描图像显示了使用虚拟多平面切片识别和追踪传导系统的可行性,分别在(A–C)对照心脏和(D–F)病变心脏中展示。在对照心脏中,窦房结和房室结紧邻周围的心房心肌、结旁区(PN)和终末嵴(TC),有多个潜在的连接点。多平面切片显示了房室结的血管连接(红色箭头在B, C, E, F中)。这些连接可见于分隔心房和心室心肌的明亮纤维组织中,代表了正常的结室连接的潜在位置。在病变心脏中,窦房结和房室结区域存在脂肪浸润,将相应的结节组织与周围的右心房(RA)心肌分开(黄色箭头在B, C, E, F中)以及结旁区。这种脂肪浸润延长了结节组织与周围心房心肌之间的连接(在D中)。特别是房室结与房间隔之间的连接(★在B, C, E, F中),作为潜在的快速通路,在病变心脏中相比对照心脏有所减少。在病变心脏的更低切片中,穿过下锥体间隙(在F中),可以看到与右心房前庭(潜在的慢通路)的连接减弱。ISR = 下隔间隙(在左心室内),LA = 左心房。

Figure 5: (A, B) Three-dimensional cinematic renderings and (C, D) images from hierarchical phase-contrast tomography (HiP-CT) show segmentation of the coronary arterial and venous tree in the diseased heart. (A) The heart is viewed on its apex to show the course of the major coronary arteries and veins as well as smaller vessels such as the sinoatrial nodal artery (SNA). The coronary vasculature is lifted away from the epicardial surface by lipomatous hypertrophy, lengthening the penetrating arteries (see also Fig 1). Box indicates the location of the stent shown in B; line indicates the cross-section shown in C. (B) Cinematic rendering of one of the coronary stents, along with surrounding calcification (purple), shows feasibility of imaging both soft and hard tissue with minimal artifacts. (C) High-spatial-resolution local tomography of the left descending coronary artery shows atherosclerotic plaque including calcification (box). (D) Digital zoom scan of box in C shows details of the atherosclerotic plaque and calcification within the intima. Adip = adipose tissue, Adv = tunica adventitia, Ao = aorta, Ath = atherosclerosis, C = calcification, LAD = left anterior descending coronary artery, Lum = lumen, Med = tunica media, RCA = right coronary artery, VV = vasa vasorum.
图5: (A, B) 三维电影渲染和 (C, D) 分层相位对比断层扫描(HiP-CT)图像显示了病变心脏中冠状动脉和静脉树的分割。(A) 心脏从其顶点视角显示主要冠状动脉和静脉的路径,以及窦房结动脉(SNA)等较小血管。冠状血管被脂肪性肥大抬离心外膜表面,延长了穿透动脉(参见图1)。方框指示了(B)中显示的支架位置;线条指示了(C)中显示的横截面。(B) 一个冠状动脉支架的电影渲染图,以及周围的钙化(紫色),显示了成像软组织和硬组织的可行性,且伪影较少。(C) 左前降支冠状动脉的高空间分辨率局部断层扫描显示了包括钙化在内的动脉粥样硬化斑块(方框)。(D) (C)中方框的数字放大扫描显示了动脉粥样硬化斑块和内膜内钙化的细节。Adip = 脂肪组织,Adv = 外膜,Ao = 主动脉,Ath = 动脉粥样硬化,C = 钙化,LAD = 左前降支冠状动脉,Lum = 管腔,Med = 中膜,RCA = 右冠状动脉,VV = 血管滋养管。
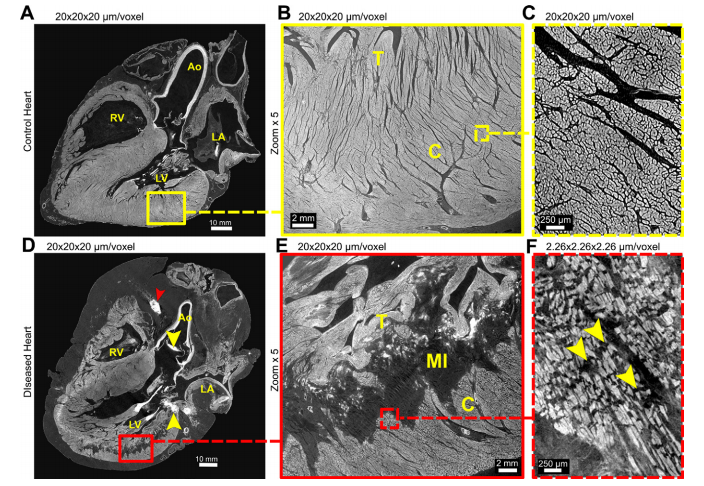
Figure 6: Hierarchical phase-contrast tomography scans of ventricular myocardium in (A–C) control and (D–F) diseased heart. (A, D) Long-axis views show the extent of myocardial infarction (MI) in the diseased heart, together with lipomatous hypertrophy, bright areas of calcification in the aortic valve and mitral annulus (yellow arrowheads in D), and stent in the right coronary artery (red arrowhead in D). (B, E) Zoom scans of boxes in A and D show the high spatial resolution obtained even at this voxel size and the extensive nature of the myocardial infarction that lies immediately beneath the trabecular myocardium (T). (C, F) High-spatial-resolution scans of the boxed areas in B and E show differences in myocardial aggregates, which are separated by replacement fibrosis in the diseased heart (yellow arrowheads in F) but tightly packed in the control heart. Ao = aorta, C = compact myocardium, LA = left atrium, LV = left ventricle, RV = right ventricle.
图6: 分层相位对比断层扫描显示了(A–C)对照心脏和(D–F)病变心脏中的心室心肌情况。(A, D) 长轴视图显示了病变心脏中心肌梗死(MI)的范围,以及脂肪性肥大、主动脉瓣和二尖瓣环中明亮的钙化区域(黄色箭头在D中)和右冠状动脉中的支架(红色箭头在D中)。(B, E) 放大扫描了A和D中的方框区域,显示即使在这种体素大小下也能获得的高空间分辨率,以及紧贴小梁心肌(T)下方的广泛心肌梗死区域。(C, F) 高空间分辨率扫描了B和E中的方框区域,显示了心肌集群的差异,对照心脏中心肌集群紧密堆积,而病变心脏中被替代性纤维化分隔(黄色箭头在F中)。Ao = 主动脉,C = 紧凑型心肌,LA = 左心房,LV = 左心室,RV = 右心室。















 339
339

 被折叠的 条评论
为什么被折叠?
被折叠的 条评论
为什么被折叠?
 到【灌水乐园】发言
到【灌水乐园】发言









