






Title
题目
Addition of Contrast-enhanced Mammography to Tomosynthesis for Breast Cancer Detection in Women with a Personal History of Breast Cancer:
将增强型乳腺摄影添加到断层合成中用于有乳腺癌个人病史女性的乳腺癌检测:
Background
背景
Digital breast tomosynthesis (DBT) is often inadequate for screening women with a personal history of breast cancer (PHBC). The ongoing prospective Tomosynthesis or Contrast-Enhanced Mammography, or TOCEM, trial includes three annual screenings with both DBT and contrast-enhanced mammography (CEM).
数字乳腺断层合成(DBT)通常不足以筛查有乳腺癌个人病史(PHBC)的女性。正在进行的前瞻性Tomosynthesis或Contrast-Enhanced Mammography(TOCEM)试验包括使用DBT和增强型乳腺摄影(CEM)进行的三次年度筛查。
Method
方法
From October 2019 to December 2022, two radiologists interpreted both examinations: Observer 1 reviewed DBT first and then CEM, and observer 2 reviewed CEM first and then DBT. Effects of adding CEM to DBT on incremental cancer detection rate (ICDR), cancer type and node status, recall rate, and other performance characteristics of the primary radiologist decisions were assessed.
从2019年10月到2022年12月,两位放射科医生对这两种检查进行了解读:观察者1先审查DBT,然后审查CEM,观察者2先审查CEM,然后审查DBT。评估将CEM添加到DBT中的增量癌症检测率(ICDR)、癌症类型和淋巴结状态、召回率以及初级放射科医生决策的其他性能特征的影响。
Conclusion
结论
CEM added to DBT increased early breast cancer detection each year in women with PHBC, with an accompanying approximately 5.0%–6.6% recall rate increase.Clinical trial registration no. NCT04085510
将CEM添加到DBT中,每年都能增加有乳腺癌个人病史(PHBC)女性的早期乳腺癌检测率,同时伴随约5.0%–6.6%的召回率增加。临床试验注册号:NCT04085510
Results
结果
Among the participants (mean age at entry, 63.6 years ± 9.6 [SD]), 1273, 819, and 227 women with PHBC completed year 1, 2, and 3 screening, respectively. For observer 1, year 1 cancer yield was 20 of 1273 (15.7 per 1000 screenings) for DBT and 29 of 1273 (22.8 per 1000 screenings; ICDR, 7.1 per 1000 screenings [95% CI: 3.2, 13.4]) for DBT plus CEM (P < .001). Year 2 plus 3 cancer yield was four of 1046 (3.8 per 1000 screenings) for DBT and eight of 1046 (7.6 per 1000 screenings; ICDR, 3.8 per 1000 screenings [95% CI: 1.0, 7.6]) for DBT plus CEM (P = .001). Year 1 recall rate for observer 1 was 103 of 1273 (8.1%) for (incidence) DBT alone and 187 of 1273 (14.7%) for DBT plus CEM (difference = 84 of 1273, 6.6% [95% CI: 5.3, 8.1]; P < .001). Year 2 plus 3 recall rate was 40 of 1046 (3.8%) for DBT and 92 of 1046 (8.8%) for DBT plus CEM (difference = 52 of 1046, 5.0% [95% CI: 3.7, 6.3]; P < .001). In 18 breasts with cancer detected only at CEM after integration of both observers, 13 (72%) cancers were invasive (median tumor size, 0.6 cm) and eight of nine (88%) with staging were N0. Among 1883 screenings with adequate reference standard, there were three interval cancers (one at the scar, two in axillae).
在参与者中(入组时的平均年龄为63.6岁±9.6 [SD]),分别有1273名、819名和227名有乳腺癌个人病史(PHBC)的女性完成了第1年、第2年和第3年的筛查。对于观察者1,第1年的癌症检出率为DBT单独筛查时1273人中有20例(每千次筛查15.7例),而DBT加CEM筛查时1273人中有29例(每千次筛查22.8例;ICDR,每千次筛查7.1例[95% CI:3.2, 13.4],P < .001)。第2年和第3年的癌症检出率为DBT单独筛查时1046人中有4例(每千次筛查3.8例),而DBT加CEM筛查时1046人中有8例(每千次筛查7.6例;ICDR,每千次筛查3.8例[95% CI:1.0, 7.6],P = .001)。观察者1在第1年的召回率为DBT单独筛查时1273人中有103例(8.1%),而DBT加CEM筛查时1273人中有187例(14.7%;差异=1273人中有84例,6.6%[95% CI:5.3, 8.1],P < .001)。第2年和第3年的召回率为DBT单独筛查时1046人中有40例(3.8%),而DBT加CEM筛查时1046人中有92例(8.8%;差异=1046人中有52例,5.0%[95% CI:3.7, 6.3],P < .001)。在整合了两位观察者后的18例仅在CEM中检测到癌症的乳房中,有13例(72%)癌症为侵袭性(肿瘤中位大小为0.6厘米),并且在进行分期的9例中有8例(88%)为N0。在1883次具有充分参考标准的筛查中,有3例间隔癌症(一例在疤痕处,两例在腋窝处)。
Figure
图
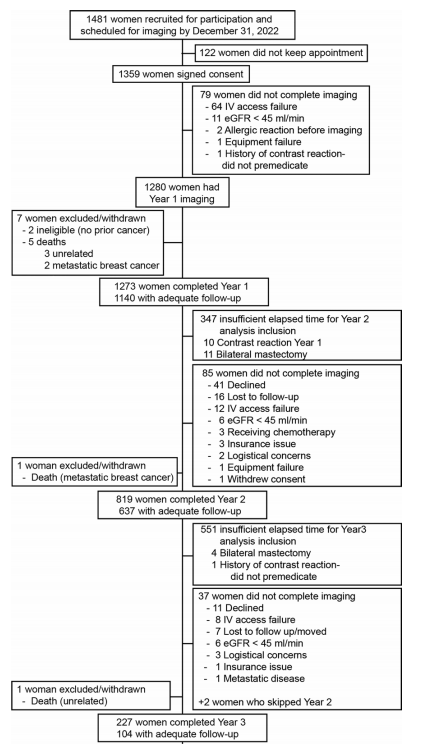
Figure 1: Flowchart of study participants. Adequate follow-up was biopsy diagnosis of cancer or no breast cancer diagnosis at surgery or follow-up imaging of at least 10.5 months, or, if no subsequent imaging or surgery had been performed, clinical follow-up of at least 12 months. Four women had mild contrast agent reactions in year 2 and planned to premedicate and continue participation, but one failed to premedicate and was excluded in year 3. eGFR = estimated glomerular filtration rate, IV = intravenous.
图1: 研究参与者流程图。充分的随访定义为活检诊断为癌症或在手术或随访影像检查中未诊断为乳腺癌,随访时间至少为10.5个月,或如果未进行后续影像检查或手术,临床随访至少为12个月。四名女性在第二年出现轻微的对比剂反应,计划预先用药后继续参与,但其中一人在第三年未能预先用药,因此被排除在外。eGFR = 估计肾小球滤过率,IV = 静脉注射。
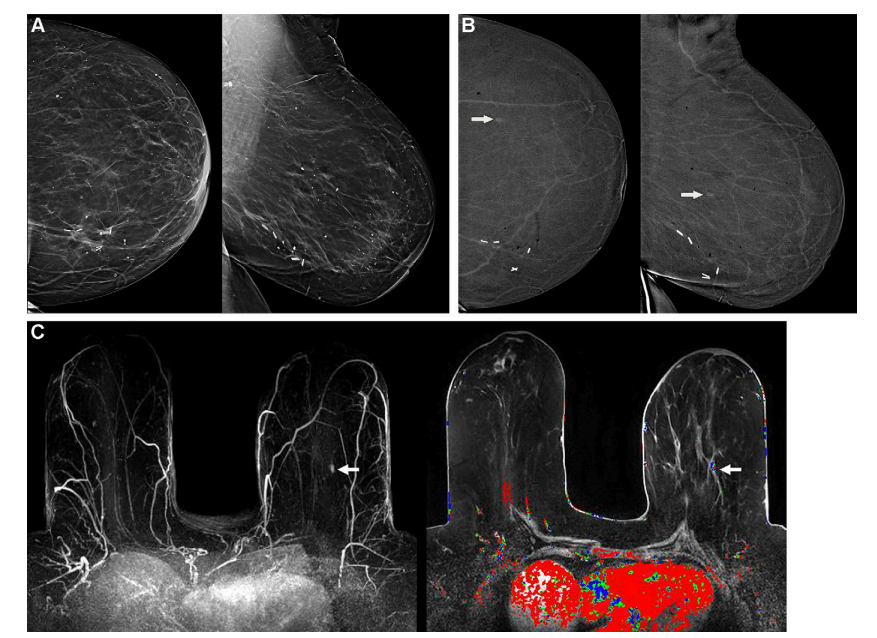
Figure 2: Images in a 67-year-old woman with triple receptor–negative invasive ductal carcinoma (IDC) seen only at contrast-enhanced mammography (CEM) at year 2. (A) Left craniocaudal (CC) (left) and mediolateral oblique (MLO) (right) low-energy images show scattered fibroglandular density and postsurgical scarring, with clips in the lower inner quadrant at the site of lumpectomy for a 2.1-cm grade 3 IDC, estrogen receptor– and progesterone receptor–positive and human epidermal growth factor receptor 2 (HER2) (ERBB2 gene)–negative lesion 11 years prior. Scattered benign-appearing calcifications are noted. The participant also completed radiation therapy and adjuvant chemotherapy and was treated with tamoxifen for 7 years and then with an aromatase inhibitor for 3 years, with last use 1 year prior to study entry. (B) Recombined CC (left) and MLO (right) CEM images obtained in year 2 show moderately conspicuous enhancement of an oval mass in the upper outer left breast (arrows), which was new from the prior CEM examination (not shown). This lesion was assessed as Breast Imaging Reporting and Data System (BI-RADS) 4B, moderately suspicious, by observer 1 and as BI-RADS 3, probably benign, but recommended for additional evaluation, by observer 2. At the time, CEM-guided biopsy was not available, so the participant underwent MRI and MRI-guided biopsy. (C) Axial maximum intensity projection from T1-weighted fat-suppressed MRI (left) shows moderately intense enhancement of the same mass (arrow), with plateau and washout kinetics (arrow) on axial post-contrast fat-suppressed T1-weighted image with kinetic overlay (right). MRI-guided biopsy and excision revealed a 0.5-cm grade 3 IDC, triple receptor–negative lesion (Ki-67 proliferation index of 55%). Three sentinel nodes were negative for metastasis.
图2: 一位67岁女性在第2年通过对比增强乳腺摄影(CEM)仅发现的三重受体阴性浸润性导管癌(IDC)影像。(A) 左侧头尾位(CC)(左)和内外侧斜位(MLO)(右)低能量图像显示分散的纤维腺体密度和手术后的疤痕,下内象限的肿块切除术部位有夹子,11年前为2.1厘米3级IDC,雌激素受体(ER)和孕激素受体(PR)阳性、人表皮生长因子受体2(HER2)阴性(ERBB2基因)病变。注意到分散的良性钙化。参与者还完成了放疗和辅助化疗,并使用他莫昔芬7年,然后使用芳香酶抑制剂3年,最后一次使用是在研究开始前1年。(B) 第2年获得的重组CC(左)和MLO(右)CEM图像显示左上外乳房椭圆形肿块中度显著增强(箭头),这是先前CEM检查的新发现(未显示)。观察者1评估该病变为乳腺影像报告和数据系统(BI-RADS)4B,怀疑中等;观察者2评估为BI-RADS 3,可能为良性,但建议进一步评估。当时没有可用的CEM引导活检,因此参与者接受了MRI和MRI引导的活检。(C) T1加权脂肪抑制MRI的轴向最大强度投影(左)显示相同肿块的中度强烈增强(箭头),在轴向对比增强脂肪抑制T1加权图像上有平台期和清洗动力学叠加(右)。MRI引导的活检和切除显示0.5厘米的3级IDC,三重受体阴性病变(Ki-67增殖指数为55%)。三个前哨淋巴结未发现转移。
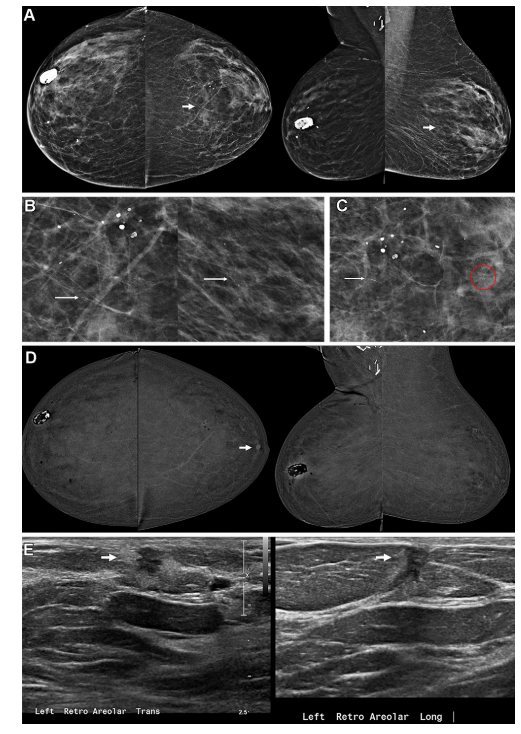
Figure 3: Images in a 77-year-old woman with invasive ductal carcinoma (IDC) seen only at contrast-enhanced mammography (CEM) and ductal carcinoma in situ (DCIS) seen only on low-energy (LE) images and digital breast tomosynthesis images at year 2. (A)Bilateral craniocaudal (CC) (left) and mediolateral oblique (MLO) (right) LE images show heterogeneously dense parenchyma and postsurgical changes with dystrophic calcifications in the upper right breast and clips in the right axilla from breast-conserving therapy for a grade 1 IDC, estrogen receptor (ER)– and progesterone receptor (PR)–positive, human epidermal growth factor receptor 2 (HER2) (ERBB2 gene)–negative, 19 years earlier, for which she had taken Anastrozole for 4 years. Only observer 1 recalled the participant for linear calcifications in the left breast (arrows), which are better seen on (B) close-up CC (left) and MLO (right) LE images (arrows) and (C) a spot magnification CC view of the central left breast. In addition to typically benign calcifications more laterally and fine linear calcifications (arrow in C), seenonly on C more anteriorly, there is a group of amorphouscalcifications (circle in C). Both areas of calcification wererecommended for biopsy, despite lack of enhancement on (D) recombined CC (left) and MLO (right) CEM images. A moderately conspicuous enhancing mass in the retroareolar left breast was newly seen, which was only evident at CC CEM (arrow in D) and was assessed as Breast Imaging Reporting and Data System (BI-RADS) 4A, low suspicion, by observer 1 and as BI-RADS 4B, moderate suspicion, by observer 2. (E) CEM-directed US images (left = transverse plane, right = longitudinal plane) of the retroareolar left breast show an irregular, hypoechoic mass (arrows) with an echogenic rim, highly suggestive of malignancy (BI-RADS 5). US-guided core biopsy and mastectomy revealed a 2.1-cm grade 3 ER and PR-positive, ERBB2-negative IDC. Stereotactic biopsy of the linear calcifications revealed high-grade ER and PR-positive DCIS, and biopsy of the amorphous calcifications yielded atypical ductal hyperplasia. At mastectomy, 5.5 cm of highnuclear-grade DCIS was found, discontinuous with the retroareolar IDC. One of two sentinel nodes showed isolated tumor cells (N0).
图3: 一位77岁女性在第2年仅通过对比增强乳腺摄影(CEM)发现浸润性导管癌(IDC)及仅通过低能量(LE)图像和数字乳腺断层合成图像发现导管原位癌(DCIS)。(A) 双侧头尾位(CC)(左)和内外侧斜位(MLO)(右)LE图像显示异质性密集的实质和术后变化,右上乳房的营养不良性钙化以及右腋窝的夹子,19年前因1级IDC接受乳房保留治疗,雌激素受体(ER)和孕激素受体(PR)阳性,人表皮生长因子受体2(HER2)(ERBB2基因)阴性,并服用了4年阿那曲唑。仅观察者1因左乳房的线性钙化(箭头)召回了参与者,这在(B)近距离CC(左)和MLO(右)LE图像(箭头)以及(C)左乳房中央的点放大CC视图中更清晰。在更外侧通常为良性的钙化和更前方的细线状钙化(*C*中的箭头)之外,还有一组无定形钙化(*C*中的圆圈)。尽管在(D)重组CC(左)和MLO(右)CEM图像上未见增强,仍建议对两处钙化进行活检。在左乳房乳晕后部位新发现一个中度显著的增强肿块,仅在CC CEM(*D*中的箭头)上可见,观察者1评估为乳腺影像报告和数据系统(BI-RADS)4A,低度怀疑,观察者2评估为BI-RADS 4B,中度怀疑。(E) CEM引导的左乳房乳晕后部超声图像(左=横向,右=纵向)显示一个不规则、低回声的肿块(箭头)伴有高回声边缘,高度怀疑恶性(BI-RADS 5)。超声引导的核心活检和乳房切除术显示一个2.1厘米的3级ER和PR阳性、ERBB2阴性IDC。线性钙化的立体定向活检显示高级别ER和PR阳性DCIS,无定形钙化的活检显示非典型导管增生。乳房切除术显示5.5厘米的高核级别DCIS,与乳晕后IDC不连续。两枚前哨淋巴结中的一个显示孤立的肿瘤细胞(N0)。
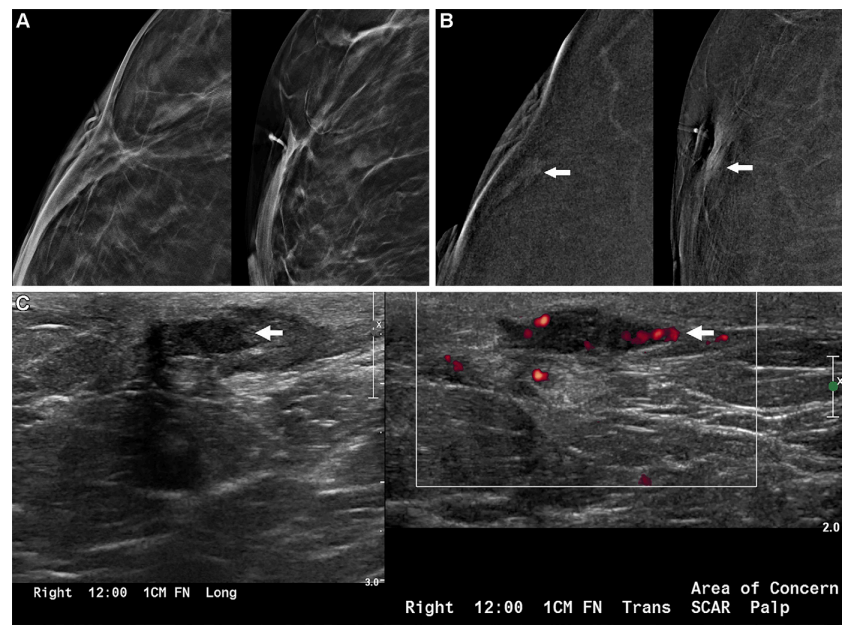
Figure 4: Images in a 47-year-old woman with recurrent invasive lobular carcinoma (ILC) at the scar detected clinically 6 months after imaging (interval cancer). (A)* Close-up craniocaudal (CC) (left) and mediolateral oblique (MLO) (right) digital breast tomosynthesis 6-mm slab images of the right breast show the area of scarring from breast-conserving therapy 2 years earlier for multifocal estrogen receptor (ER)/progesterone receptor (PR)-positive, human epidermal growth factor receptor 2 (HER2) (ERBB2 gene)–positive ILC, interpreted as benign, Breast Imaging Reporting and Data System (BI-RADS) 2, by both observers. The participant completed both neoadjuvant and adjuvant chemotherapy and was taking tamoxifen. (B) Close-up CC (left) and MLO (right) recombined contrast-enhanced mammography (CEM) images show nonmass enhancement at the scar (arrows), interpreted as benign, BI-RADS 2, by both observers. (C) US scan in longitudinal plane (left) obtained 6 months later, when theparticipant reported feeling a lump at the scar, shows a superficial irregular, parallel, hypoechoic mass (arrow) at the scar; the mass shows internal vascularity on transverse power Doppler scan (right, arrow). US-guided core biopsy and mastectomy revealed a 2.4-cm grade 3 ILC, ER-positive, PR-negative, HER2-positive lesion (Ki-67 proliferation index of 90%), with one of two sentinel nodes showing isolated tumor cells (N0).
图4: 一位47岁女性在疤痕处临床发现复发性浸润性小叶癌(ILC),影像检查后6个月(间隔癌)。(A) 近距离头尾位(CC)(左)和内外侧斜位(MLO)(右)数字乳腺断层合成的6毫米薄片图像显示右乳房在2年前因多灶性雌激素受体(ER)/孕激素受体(PR)阳性、人表皮生长因子受体2(HER2)(ERBB2基因)阳性ILC接受乳房保留治疗后的疤痕区,两个观察者均解释为良性(乳腺影像报告和数据系统BI-RADS 2)。参与者完成了新辅助和辅助化疗,并服用他莫昔芬。(B) 近距离CC(左)和MLO(右)重组的对比增强乳腺摄影(CEM)图像显示疤痕处的非肿块增强(箭头),两个观察者均解释为良性(BI-RADS 2)。(C) 6个月后,当参与者报告在疤痕处感觉到一个肿块时,获得的纵向平面超声扫描(左)显示疤痕处有一个表浅的不规则、平行、低回声的肿块(箭头);横向功率多普勒扫描(右,箭头)显示肿块内部有血管。超声引导的核心活检和乳房切除术显示一个2.4厘米的3级ILC,ER阳性,PR阴性,HER2阳性病变(Ki-67增殖指数为90%),两个前哨淋巴结中的一个显示孤立的肿瘤细胞(N0)。
Table
表
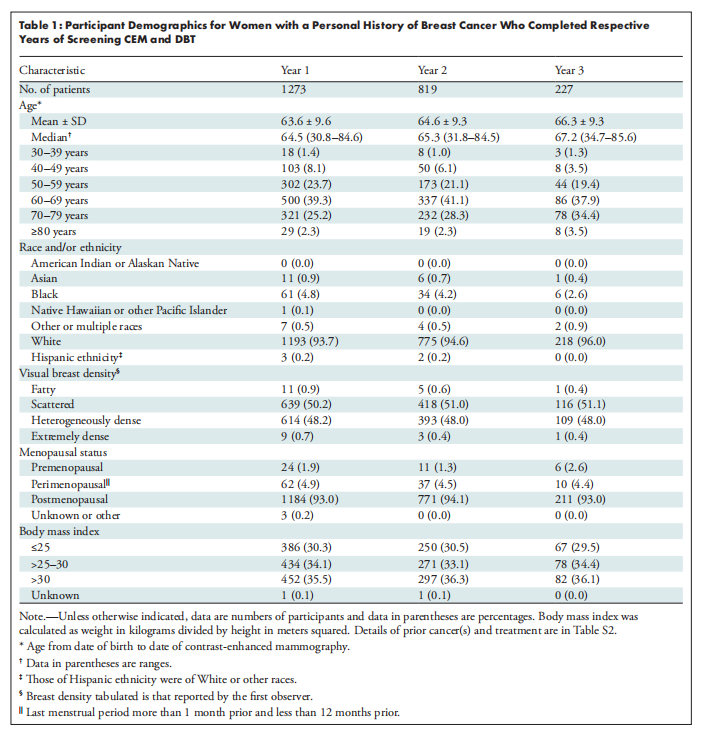
Table 1: Participant Demographics for Women with a Personal History of Breast Cancer Who Completed Respective Years of Screening CEM and DBT
表1: 完成各年份CEM和DBT筛查的有乳腺癌个人病史女性的参与者人口统计数据
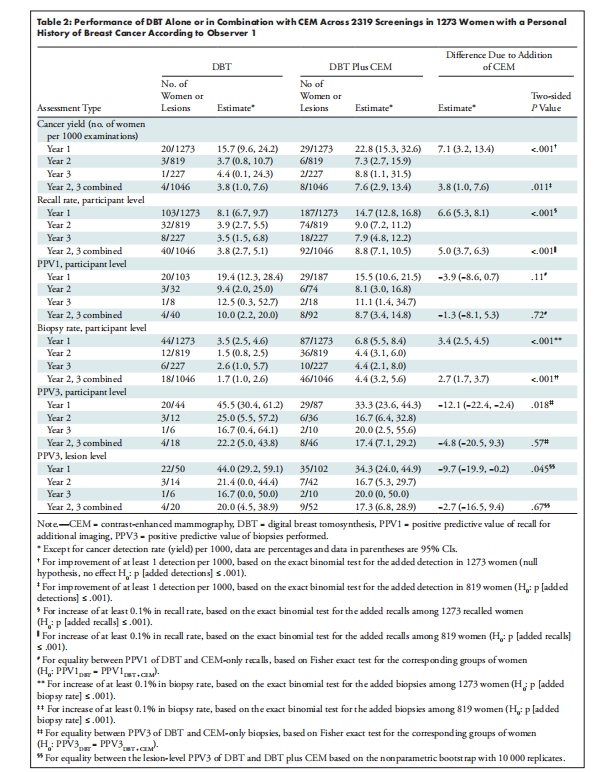
Table 2: Performance of DBT Alone or in Combination with CEM Across 2319 Screenings in 1273 Women with a Personal History of Breast Cancer According to Observer 1
表2: 根据观察者1,2319次筛查中1273名有乳腺癌个人病史女性使用DBT单独或联合CEM的表现
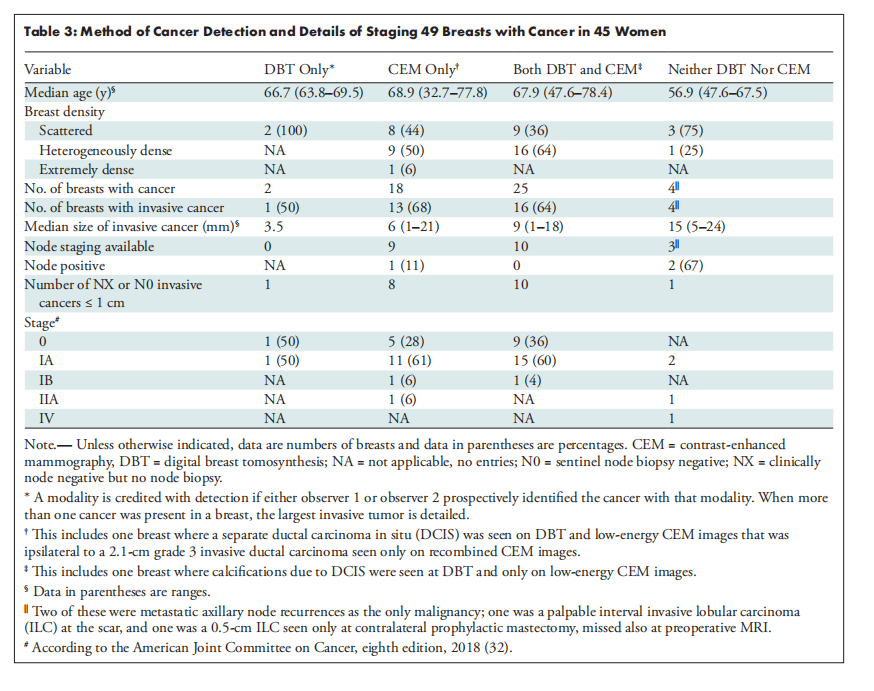
Table 3: Method of Cancer Detection and Details of Staging 49 Breasts with Cancer in 45 Women
表3: 45名女性中49个癌症乳房的癌症检测方法和分期详情















 1827
1827

 被折叠的 条评论
为什么被折叠?
被折叠的 条评论
为什么被折叠?
 到【灌水乐园】发言
到【灌水乐园】发言









